

Neurological and autoimmune disorders after vaccination against pandemic influenza A (H1N1) with a monovalent adjuvanted vaccine: population based cohort study in Stockholm, Sweden
- PMID: 21994316
- PMCID: PMC3192001
- DOI: 10.1136/bmj.d5956
Neurological and autoimmune disorders after vaccination against pandemic influenza A (H1N1) with a monovalent adjuvanted vaccine: population based cohort study in Stockholm, Sweden
Abstract
Objective: To examine the risk of neurological and autoimmune disorders of special interest in people vaccinated against pandemic influenza A (H1N1) with Pandemrix (GlaxoSmithKline, Middlesex, UK) compared with unvaccinated people over 8-10 months.
Design: Retrospective cohort study linking individualised data on pandemic vaccinations to an inpatient and specialist database on healthcare utilisation in Stockholm county for follow-up during and after the pandemic period.
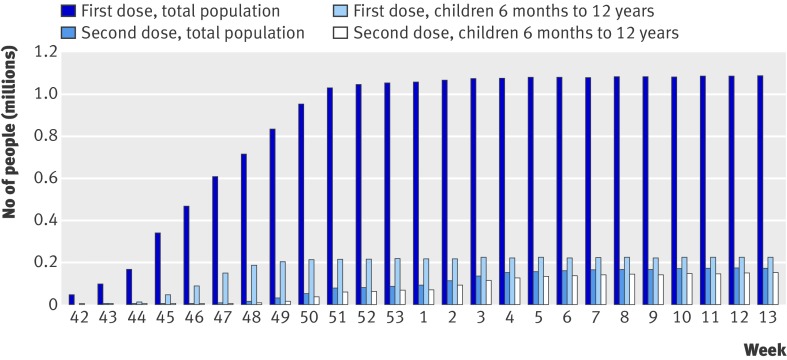
Setting: Stockholm county, Sweden. Population All people registered in Stockholm county on 1 October 2009 and who had lived in this region since 1 January 1998; 1,024,019 were vaccinated against H1N1 and 921,005 remained unvaccinated.
Main outcome measures: Neurological and autoimmune diagnoses according to the European Medicines Agency strategy for monitoring of adverse events of special interest defined using ICD-10 codes for Guillain-Barré syndrome, Bell's palsy, multiple sclerosis, polyneuropathy, anaesthesia or hypoaesthesia, paraesthesia, narcolepsy (added), and autoimmune conditions such as rheumatoid arthritis, inflammatory bowel disease, and type 1 diabetes; and short term mortality according to vaccination status.
Results: Excess risks among vaccinated compared with unvaccinated people were of low magnitude for Bell's palsy (hazard ratio 1.25, 95% confidence interval 1.06 to 1.48) and paraesthesia (1.11, 1.00 to 1.23) after adjustment for age, sex, socioeconomic status, and healthcare utilisation. Risks for Guillain-Barré syndrome, multiple sclerosis, type 1 diabetes, and rheumatoid arthritis remained unchanged. The risks of paraesthesia and inflammatory bowel disease among those vaccinated in the early phase (within 45 days from 1 October 2009) of the vaccination campaign were significantly increased; the risk being increased within the first six weeks after vaccination. Those vaccinated in the early phase were at a slightly reduced risk of death than those who were unvaccinated (0.94, 0.91 to 0.98), whereas those vaccinated in the late phase had an overall reduced mortality (0.68, 0.64 to 0.71). These associations could be real or explained, partly or entirely, by residual confounding.
Conclusions: Results for the safety of Pandemrix over 8-10 months of follow-up were reassuring -notably, no change in the risk for Guillain-Barré syndrome, multiple sclerosis, type 1 diabetes, or rheumatoid arthritis. Relative risks were significantly increased for Bell's palsy, paraesthesia, and inflammatory bowel disease after vaccination, predominantly in the early phase of the vaccination campaign. Small numbers of children and adolescents with narcolepsy precluded any meaningful conclusions.
Conflict of interest statement
Competing interests: All authors have completed the ICMJE uniform disclosure form at
Figures
References
-
- World Health Organization. New influenza A (H1N1) virus; global epidemiological situation. Wkly Epidemiol Rec 2009;84:249-57. - PubMed
-
- Johansen K, Nicoll A, Ciancio BC, Kramarz P. Pandemic influenza A(H1N1) 2009 vaccines in the European Union. Euro Surveill 2009;14:19361. - PubMed
-
- World Health Organization. Influenza pandemic preparedness and response. Report by the secretariat. WHO, 2005.
-
- Diez-Domingo J, Garcés-Sanchez M, Baldó JM, Planelles MV, Ubeda I, JuBert A, et al. Immunogenecity and safety of H5N1 A/Vietnam/1194/2004 (Clade 1) AS03-adjuvanted prepandemic candidate influenza vaccines in children aged 3 to 9 years: a phase ii, randomized, open, controlled study. Pediatr Infect Dis J 2010;29:e35-46. - PubMed
-
- Schwarz TF, Horacek T, Knuf M, Damman HG, Roman F, Dramé M, et al. Single dose vaccination with AS03-adjuvanted H5N1 vaccines in a randomized trial induces strong and broad immune responsiveness to booster vaccination in adults. Vaccine 2009;27:6284-90. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical