

Variations of oral microbiota are associated with pancreatic diseases including pancreatic cancer
- PMID: 21994333
- PMCID: PMC3705763
- DOI: 10.1136/gutjnl-2011-300784
Variations of oral microbiota are associated with pancreatic diseases including pancreatic cancer
Abstract
Objective: The associations between oral diseases and increased risk of pancreatic cancer have been reported in several prospective cohort studies. In this study, we measured variations of salivary microbiota and evaluated their potential associations with pancreatic cancer and chronic pancreatitis.
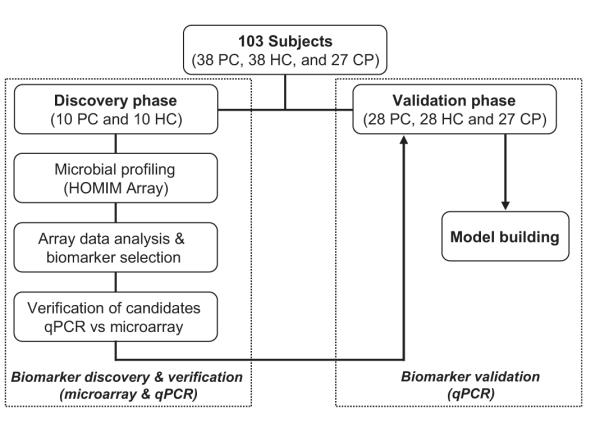
Methods: This study was divided into three phases: (1) microbial profiling using the Human Oral Microbe Identification Microarray to investigate salivary microbiota variation between 10 resectable patients with pancreatic cancer and 10 matched healthy controls, (2) identification and verification of bacterial candidates by real-time quantitative PCR (qPCR) and (3) validation of bacterial candidates by qPCR on an independent cohort of 28 resectable pancreatic cancer, 28 matched healthy control and 27 chronic pancreatitis samples.
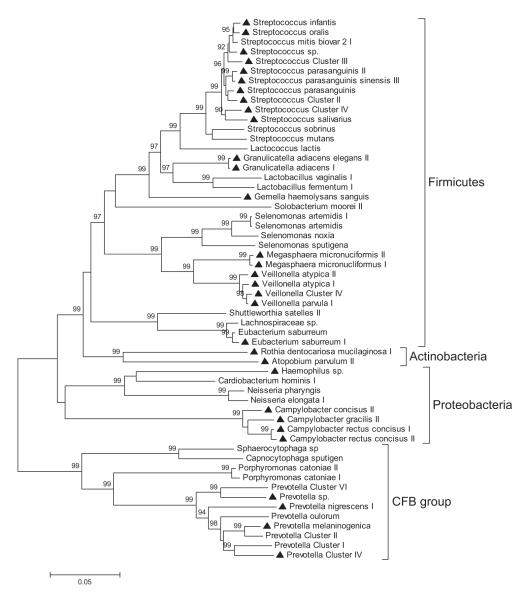
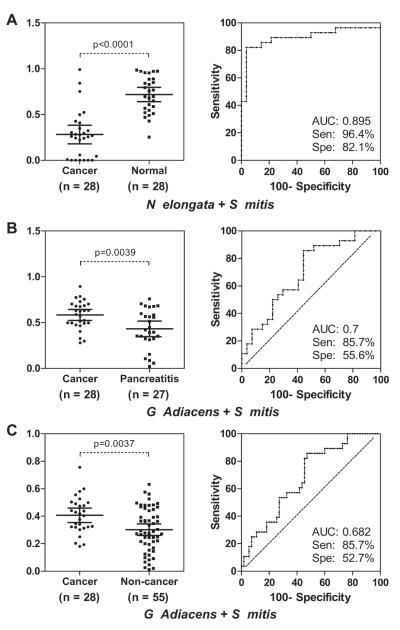
Results: Comprehensive comparison of the salivary microbiota between patients with pancreatic cancer and healthy control subjects revealed a significant variation of salivary microflora. Thirty-one bacterial species/clusters were increased in the saliva of patients with pancreatic cancer (n=10) in comparison to those of the healthy controls (n=10), whereas 25 bacterial species/clusters were decreased. Two out of six bacterial candidates (Neisseria elongata and Streptococcus mitis) were validated using the independent samples, showing significant variation (p<0.05, qPCR) between patients with pancreatic cancer and controls (n=56). Additionally, two bacteria (Granulicatella adiacens and S mitis) showed significant variation (p<0.05, qPCR) between chronic pancreatitis samples and controls (n=55). The combination of two bacterial biomarkers (N elongata and S mitis) yielded a receiver operating characteristic plot area under the curve value of 0.90 (95% CI 0.78 to 0.96, p<0.0001) with a 96.4% sensitivity and 82.1% specificity in distinguishing patients with pancreatic cancer from healthy subjects.
Conclusions: The authors observed associations between variations of patients' salivary microbiota with pancreatic cancer and chronic pancreatitis. This report also provides proof of salivary microbiota as an informative source for discovering non-invasive biomarkers of systemic diseases.
Figures
Comment in
-
Pancreas: Oral microbiota and pancreatic disease.Nat Rev Gastroenterol Hepatol. 2011 Nov 15;8(12):659. doi: 10.1038/nrgastro.2011.206. Nat Rev Gastroenterol Hepatol. 2011. PMID: 22083124 No abstract available.
References
-
- Hezel AF, Kimmelman AC, Stanger BZ, et al. Genetics and biology of pancreatic ductal adenocarcinoma. Genes Dev. 2006;20:1218–49. - PubMed
-
- Whitcomb DC. Inflammation and cancer V. Chronic pancreatitis and pancreatic cancer. Am J Physiol Gastrointest Liver Physiol. 2004;287:G315–19. - PubMed
-
- Li D, Xie K, Wolff R, et al. Pancreatic cancer. Lancet. 2004;363:1049–57. - PubMed
-
- Jemal A, Siegel R, Ward E, et al. Cancer statistics, 2008. CA Cancer J Clin. 2008;58:71–e96. - PubMed
-
- Ries LAG, Melbert D, Krapcho M, et al. SEER cancer statistics review, 1975–2005, National Cancer Institute. SEER data submission, posted to the SEER website; Bethesda, MD: 2008. based on November 2007. http://seer.cancer.gov/csr/1975_2005/
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical