

Application Of The American College Of Emergency Physicians (ACEP) Recommendations And a Risk Stratification Score (OESIL) For Patients With Syncope Admitted From The Emergency Department
- PMID: 21994471
- PMCID: PMC3184449
Application Of The American College Of Emergency Physicians (ACEP) Recommendations And a Risk Stratification Score (OESIL) For Patients With Syncope Admitted From The Emergency Department
Abstract
Aims: The goals of this study were to apply the 2001 ACEP recommendations for admission to hospital after a syncopal event and to validate the OESIL risk stratification score, in patients with syncope admitted to a general internal medicine ward.
Methods: A retrospective study applied the 2001 ACEP recommendations and OESIL score to all the patients admitted from the emergency department to a general internal medicine ward with a diagnosis of syncope during a 12-month period. The patients were classified as meeting criteria for 2001 ACEP class B or C recommendations and OESIL score 0-1 (low-risk for a major cardiac event) or 2-4 (high-risk for a major cardiac event). The sensitivity and specificity of each group for predicting high-risk patients was calculated.
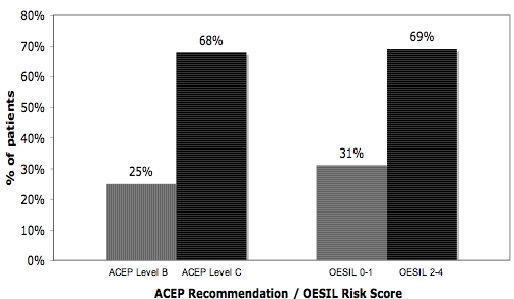
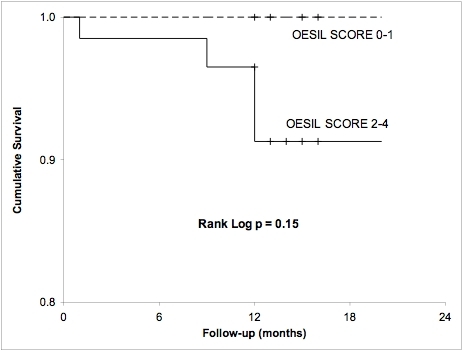
Results: After applying the 2001 ACEP recommendations to our population, 25% (19 patients) were classified as level B, whereas 68% of the patients were classified as Level C. Sensitivity for ACEP level B recommendations was 100% and specificity was 81%. The ACEP level C recommendations also had 100% sensitivity but markedly reduced specificity at 26%. An OESIL score of 0-1 points was calculated for 30.6% of the population, identifying them as low-risk. An OESIL score of 2-4 points was documented in the remaining 69.4% with a mortality risk of 20 % /year.
Conclusion: A significant proportion (30%) of patients presenting with syncope to a tertiary care University Hospital emergency department and admitted to an Internal Medicine ward were retrospectively classified as low-risk and could have potentially been managed as outpatients. Implementing current guidelines and clinical pathways for the management of syncope may improve this approach.
Keywords: ACEP recommendations; OESIL score; Syncope.
Figures
References
-
- American College of Emergency Physicians Clinical Policies Subcommittee on Syncope, et al. Clinical Policy: Critical Issues in the Evaluation and Management of Adult Patients Presenting to the Emergency Department with Syncope. Ann Emerg Med. 2007;49:431. - PubMed
-
- Sun BC, et al. Characteristics and admission patterns of patients presenting with syncope to U.S. emergency departments, 1992-2000. Acad Emerg Med. 2004;11:1029. - PubMed
-
- Brignole M, et al. Guidelines on management (diagnosis and treatment) of syncope. Eur Heart J. 2001;22:1256. - PubMed
-
- Ammirati F, et al. Diagnosing syncope in the clinical practice. Implementation of a simplified diagnostic algorithm in a multicentre prospective trial - the OESIL 2 Study (Osservatorio Epidemioologico dell Sincope nel Lazio) Eur Heart J. 2000;21:935. - PubMed
-
- Sheldon R, et al. Diagnostic criteria for vasovagal syncope based on a quantitative history. Eur Heart J . 2006;27:344. - PubMed
LinkOut - more resources
Full Text Sources