

A large sustained endemic outbreak of multiresistant Pseudomonas aeruginosa: a new epidemiological scenario for nosocomial acquisition
- PMID: 21995287
- PMCID: PMC3203071
- DOI: 10.1186/1471-2334-11-272
A large sustained endemic outbreak of multiresistant Pseudomonas aeruginosa: a new epidemiological scenario for nosocomial acquisition
Abstract
Background: Studies of recent hospital outbreaks caused by multiresistant P.aeruginosa (MRPA) have often failed to identify a specific environmental reservoir. We describe an outbreak due to a single clone of multiresistant (MR) Pseudomonas aeruginosa (PA) and evaluate the effectiveness of the surveillance procedures and control measures applied.
Methods: Patients with MRPA isolates were prospectively identified (January 2006-May 2008). A combined surveillance procedure (environmental survey, and active surveillance program in intensive care units [ICUs]) and an infection control strategy (closure of ICU and urology wards for decontamination, strict compliance with cross-transmission prevention protocols, and a program restricting the use of carbapenems in the ICUs) was designed and implemented.
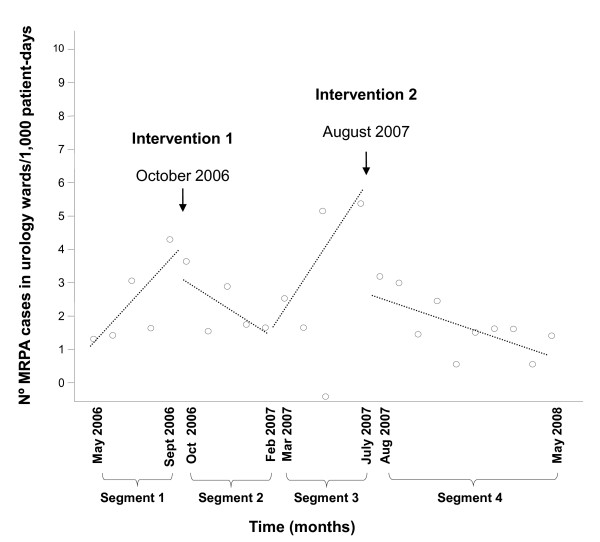
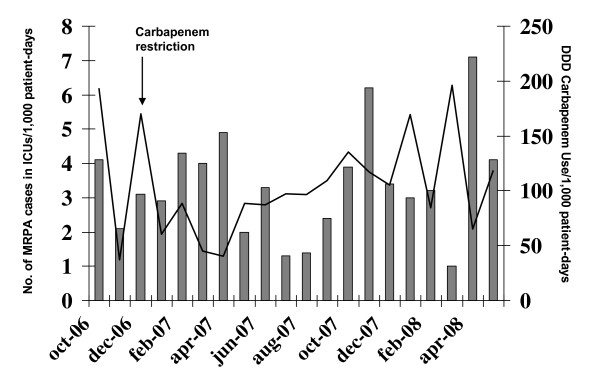
Results: Three hundred and ninety patients were identified. ICU patients were the most numerous group (22%) followed by urology patients (18%). Environmental surveillance found that 3/19 (16%) non-ICU environmental samples and 4/63 (6%) ICU samples were positive for the MRPA clonal strain. In addition, active surveillance found that 19% of patients were fecal carriers of MRPA. Significant changes in the trends of incidence rates were noted after intervention 1 (reinforcement of cleaning procedures): -1.16 cases/1,000 patient-days (95%CI -1.86 to -0.46; p = 0.003) and intervention 2 (extensive decontamination): -1.36 cases/1,000 patient-days (95%CI -1.88 to -0.84; p < 0.001) in urology wards. In addition, restricted use of carbapenems was initiated in ICUs (January 2007), and their administration decreased from 190-170 DDD/1,000 patient-days (October-December 2006) to 40-60 DDD/1,000 patient-days (January-April 2007), with a reduction from 3.1 cases/1,000 patient-days in December 2006 to 2.0 cases/1,000 patient-days in May 2007. The level of initial carbapenem use rose again during 2008, and the incidence of MRPA increased progressively once more.
Conclusions: In the setting of sustained MRPA outbreaks, epidemiological findings suggest that patients may be a reservoir for further environmental contamination and cross-transmission. Although our control program was not successful in ending the outbreak, we think that our experience provides useful guidance for future approaches to this problem.
Figures
References
-
- Bonten M, Bergmans D, Speijer H, Stobberingh E. Characteristics of polyclonal endemicity of Pseudomonas aeruginosa colonization in Intensive Care Units. Am J Respir Crit Care Med. 1999;160:1212–1219. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
