

Evidence for intranasal antinuclear autoantibodies in patients with chronic rhinosinusitis with nasal polyps
- PMID: 21996343
- PMCID: PMC3384688
- DOI: 10.1016/j.jaci.2011.08.037
Evidence for intranasal antinuclear autoantibodies in patients with chronic rhinosinusitis with nasal polyps
Abstract
Background: Chronic rhinosinusitis (CRS) with nasal polyps is an inflammatory condition of the nasal passage and paranasal sinuses characterized by T(H)2-biased inflammation with increased levels of B-cell activating factor of the TNF family (BAFF), B lymphocytes, and immunoglobulins. Because high levels of BAFF are associated with autoimmune diseases, we assessed for evidence of autoimmunity in patients with CRS.
Objectives: The objective of this study was to investigate the presence of autoantibodies in sinonasal tissue from patients with CRS.
Methods: Standardized nasal tissue specimens were collected from patients with CRS and control subjects and assayed for immunoglobulin production, autoantibody levels, tissue distribution of immunoglobulins, and binding potential of antibodies in nasal tissue with a multiplexed autoantibody microarray, ELISA, and immunofluorescence.
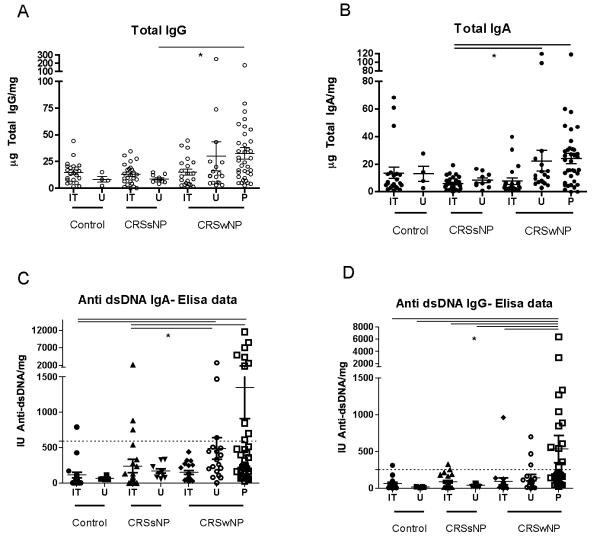
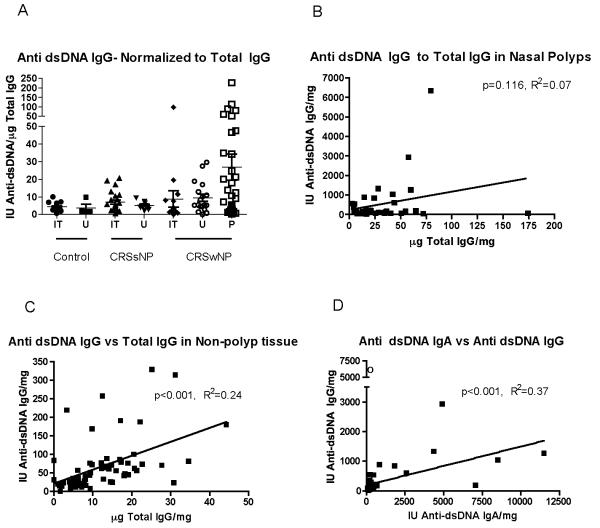
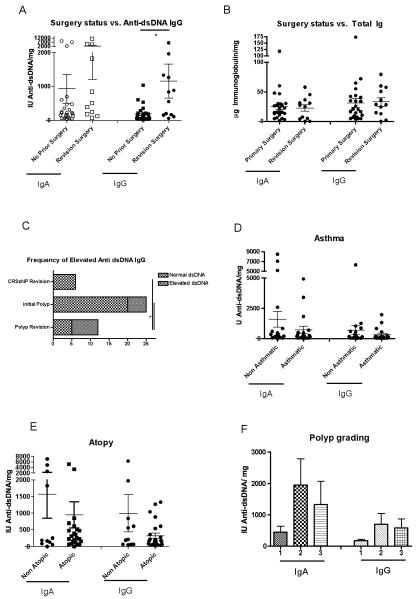
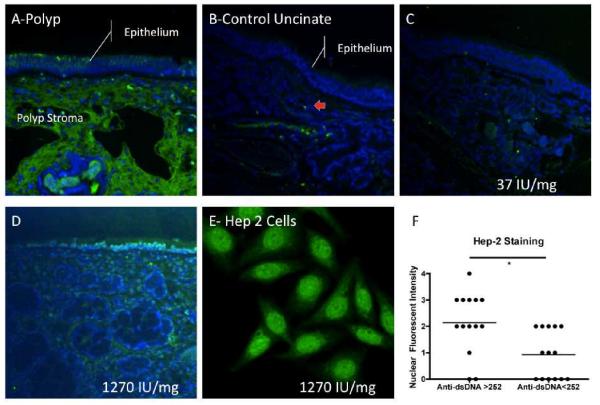
Results: Increased levels of several specific autoantibodies were found in nasal polyp tissue in comparison with levels seen in control tissue and inflamed tissue from patients with CRS without nasal polyps (P < .05). In particular, nuclear-targeted autoantibodies, such as anti-dsDNA IgG and IgA antibodies, were found at increased levels in nasal polyps (P < .05) and particularly in nasal polyps from patients requiring revision surgery for recurrence. Direct immunofluorescence staining demonstrated diffuse epithelial and subepithelial deposition of IgG and increased numbers of IgA-secreting plasma cells not seen in control nasal tissue.
Conclusions: Autoantibodies, particularly those against nuclear antigens, are present at locally increased levels in nasal polyps. The presence of autoantibodies suggests that the microenvironment of a nasal polyp promotes the expansion of self-reactive B-cell clones. Although the pathogenicity of these antibodies remains to be elucidated, the presence of increased anti-dsDNA antibody levels is associated with a clinically more aggressive form of CRS with nasal polyps requiring repeated surgery.
Copyright © 2011 American Academy of Allergy, Asthma & Immunology. Published by Mosby, Inc. All rights reserved.
Figures
References
-
- Huvenne W, van Bruaene N, Zhang N, van Zele T, Patou J, Gevaert P, et al. Chronic rhinosinusitis with and without nasal polyps: what is the difference? Curr Allergy Asthma Rep. 2009;9:213–20. - PubMed
-
- Hissaria P, Smith W, Wormald PJ, Taylor J, Vadas M, Gillis D, et al. Short course of systemic corticosteroids in sinonasal polyposis: a double-blind, randomized, placebo-controlled trial with evaluation of outcome measures. J Allergy Clin Immunol. 2006;118:128–33. - PubMed
-
- Van Zele T, Gevaert P, Holtappels G, Beule A, Wormald PJ, Mayr S, et al. Oral steroids and doxycycline: two different approaches to treat nasal polyps. J Allergy Clin Immunol. 2010;125:1069–76. e4. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
