

Outcomes among black patients with stage II and III colon cancer receiving chemotherapy: an analysis of ACCENT adjuvant trials
- PMID: 21997132
- PMCID: PMC3196480
- DOI: 10.1093/jnci/djr310
Outcomes among black patients with stage II and III colon cancer receiving chemotherapy: an analysis of ACCENT adjuvant trials
Abstract
Background: Among patients with resected colon cancer, black patients have worse survival than whites. We investigated whether disparities in survival and related endpoints would persist when patients were treated with identical therapies in controlled clinical trials.
Methods: We assessed 14,611 patients (1218 black and 13,393 white) who received standardized adjuvant treatment in 12 randomized controlled clinical trials conducted in North America for resected stage II and stage III colon cancer between 1977 and 2002. Individual patient data on covariates and outcomes were extracted from the Adjuvant Colon Cancer ENdpoinTs (ACCENT) database. The endpoints examined in this meta-analysis were overall survival (time to death), recurrence-free survival (time to recurrence or death), and recurrence-free interval (time to recurrence). Cox models were stratified by study and controlled for sex, stage, age, and treatment to determine the effect of race. Kaplan-Meier estimates were adjusted for similar covariates to control for confounding. All statistical tests were two-sided.
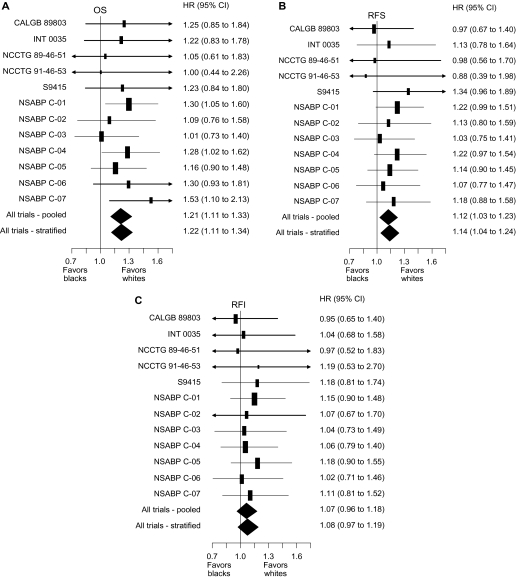
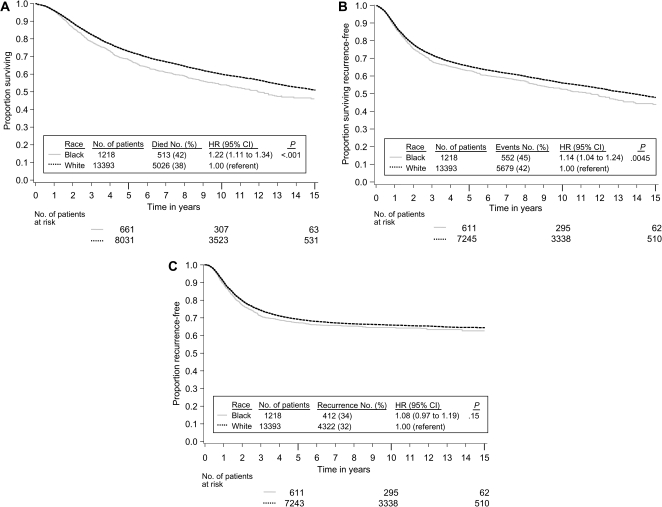
Results: Black patients were younger than whites (median age, 58 vs 61 years, respectively; P < .001) and more likely to be female (55% vs 45%, respectively; P < .001). Overall survival was worse in black patients than whites (hazard ratio [HR] of death = 1.22, 95% confidence interval [CI] = 1.11 to 1.34, P < .001). Five-year overall survival rates for blacks and whites were 68.2% and 72.8%, respectively. When subsets defined by sex, stage, and age were analyzed, overall survival was consistently worse in black patients. Recurrence-free survival was worse in black patients than whites (HR of recurrence or death = 1.14, 95% CI = 1.04 to 1.24, P = .0045). Three-year recurrence-free survival rates in blacks and whites were 68.4% and 72.1%, respectively. In contrast, recurrence-free interval was similar in black and white patients (HR of recurrence = 1.08, 95% CI = 0.97 to 1.19, P = .15). Three-year recurrence-free interval rates in blacks and whites were 71.3% and 74.2%, respectively.
Conclusions: Black patients with resected stage II and stage III colon cancer who were treated with the same therapy as white patients experienced worse overall and recurrence-free survival, but similar recurrence-free interval, compared with white patients. The differences in survival may be mostly because of factors unrelated to the patients' adjuvant colon cancer treatment.
Trial registration: ClinicalTrials.gov NCT00002593 NCT00003835 NCT00004931 NCT00096278 NCT00425152.
Figures
Comment in
-
Race and subset analyses in clinical trials: time to get serious about data integration.J Natl Cancer Inst. 2011 Oct 19;103(20):1486-8. doi: 10.1093/jnci/djr382. Epub 2011 Oct 12. J Natl Cancer Inst. 2011. PMID: 21997133 Free PMC article. No abstract available.
References
-
- Horner MJ, Ries LAG, Krapcho M, et al., editors. SEER Cancer Statistics Review, 19752006. Bethesda, MD: National Cancer Institute; 2008. http://seer.cancer.gov/csr/1975_2006/. Accessed June 1, 2010. Based on November 2008 SEER data submission, posted to the SEER web site, 2009.
-
- Polite BN, Dignam JJ, Olopade OI. Colorectal cancer and race: understanding the differences in outcomes between African Americans and whites. Med Clin North Am. 2005;89(4):771–793. - PubMed
-
- Saltz LB, Niedzwiecki D, Hollis D, et al. Irinotecan fluorouracil plus leucovorin is not superior to fluorouracil plus leucovorin alone as adjuvant treatment for stage III colon cancer: results of CALGB 89803. J Clin Oncol. 2007;25(23):3456–3461. - PubMed
-
- Moertel CG, Fleming TR, Macdonald JS, et al. Levamisole and fluorouracil for adjuvant therapy of resected colon carcinoma. N Engl J Med. 1990;322(6):352–358. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
