

Outcomes of stable HIV-positive patients down-referred from a doctor-managed antiretroviral therapy clinic to a nurse-managed primary health clinic for monitoring and treatment
- PMID: 21997488
- PMCID: PMC3669640
- DOI: 10.1097/QAD.0b013e32834b6480
Outcomes of stable HIV-positive patients down-referred from a doctor-managed antiretroviral therapy clinic to a nurse-managed primary health clinic for monitoring and treatment
Abstract
Objective: To compare clinical, immunologic and virologic outcomes among stable HIV-positive patients down-referred to a nurse-managed primary healthcare clinic (PHC) for treatment maintenance to those who remained at a doctor-managed treatment-initiation site.
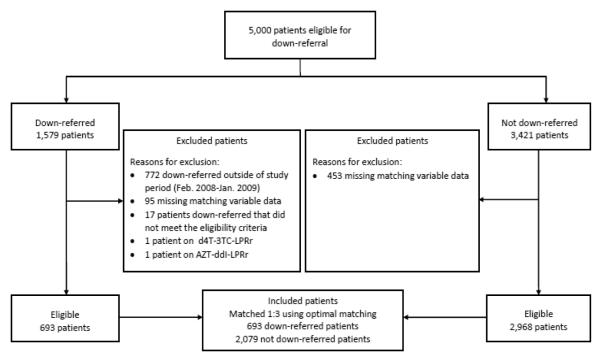
Design: We conducted a matched cohort analysis among stable HIV patients at the Themba Lethu Clinic in Johannesburg, South Africa. Eligible patients met the criteria for down-referral [undetectable viral load <10 months, antiretroviral therapy (ART) >11 months, CD4 cell count ≥200 cells/μl, stable weight and no opportunistic infections], regardless of whether they were down-referred to a PHC for treatment maintenance between February 2008 and January 2009. Patients were matched 1 : 3 (down-referred : treatment-initiation) using propensity scores.
Methods: We calculated rates and hazard ratios (HRs) for the effect of down-referral on loss to follow-up (LTFU) and mortality and the relative risk of down-referral on viral rebound by 12 months of follow-up.
Results: Six hundred and ninety-three down-referred patients were matched to 2079 treatment-initiation patients. Two (0.3%) down-referred and 32 (1.5%) treatment-initiation patients died, 10 (1.4%) down-referred and 87 (4.2%) treatment-initiation patients were lost, and 22 (3.3%) down-referred and 100 (5.6%) treatment-initiation patients experienced viral rebound by 12 months of follow-up. After adjustment, patients down-referred were less likely to die [hazard ratio (HR) 0.2, 95% confidence interval (CI) 0.04-0.8], become LTFU (HR 0.3, 95% CI 0.2-0.6) or experience viral rebound (relative risk 0.6, 95% CI 0.4-0.9) than treatment-initiation patients during follow-up.
Conclusion: The utilization of nurse-managed PHCs for treatment maintenance of stable patients could decrease the burden on specialized doctor-managed ART clinics. Patient outcomes for down-referred patients at PHCs appear equal, if not better, than those achieved at ART clinics among stable patients.
Figures

References
-
- WHO/UNAIDS/UNICEF Towards Universal Access: Scaling up priority HIV/AIDS Interventions in the Health Sector. 2010.
-
- [revision, 2010];WHO ART for HIV infection in adults and adolescents. Recommendations for a public health approach. [ http://whqlibdoc.who.int/publications/2010/9789241599764_eng.pdf] - PubMed
-
- Curran J, Debas H, Arya M, Kelley P, Knobler S, Pray L. Scaling up treatment for the global AIDS pandemic: challenges and opportunities. National Academies Press; Washington: 2005. - PubMed
-
- Dhaliwal M, Ellman T. Improving access to anti-retroviral treatment in Cambodia. International HIV/AIDS Alliance; Brighton: 2003.
-
- Gilks C, Crowley S, Ekpini R, Gove S, Perriens J, Souteyrand Y. The WHO public-health approach to antiretroviral treatment against HIV in resource-limited settings. Lancet. 2006;368(9534):505–510. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
