

Nodular lymphocyte-predominant hodgkin lymphoma with atypical T cells: a morphologic variant mimicking peripheral T-cell lymphoma
- PMID: 21997687
- PMCID: PMC6324169
- DOI: 10.1097/PAS.0b013e31822832de
Nodular lymphocyte-predominant hodgkin lymphoma with atypical T cells: a morphologic variant mimicking peripheral T-cell lymphoma
Abstract
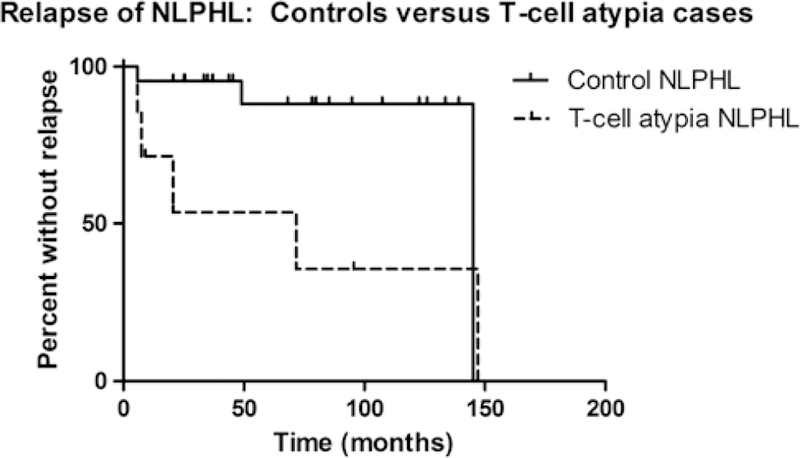
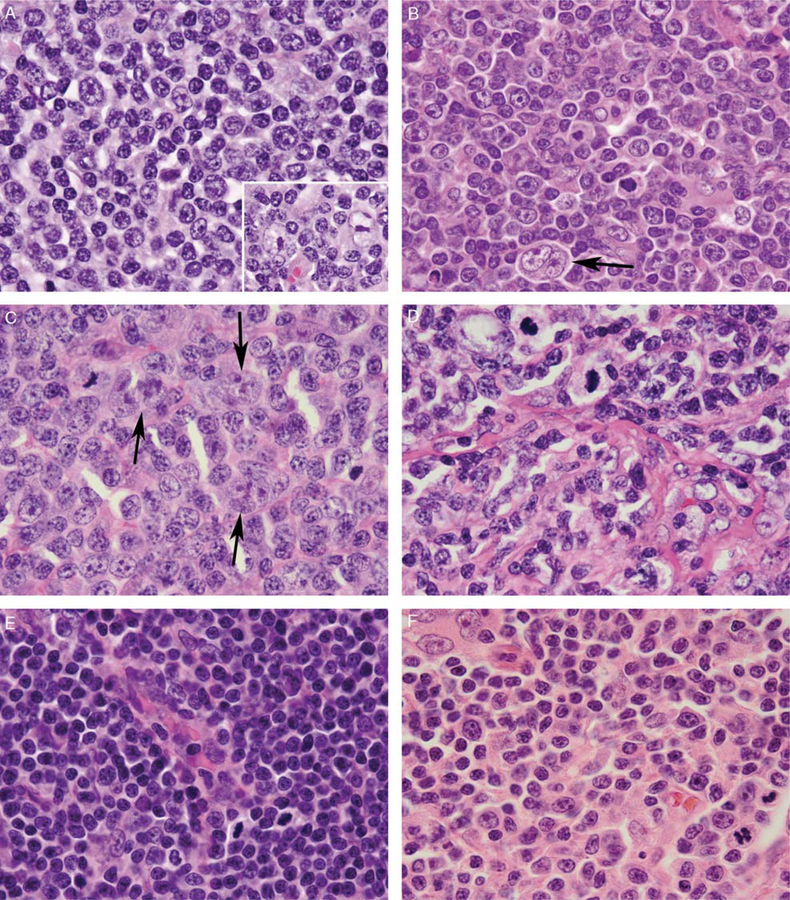
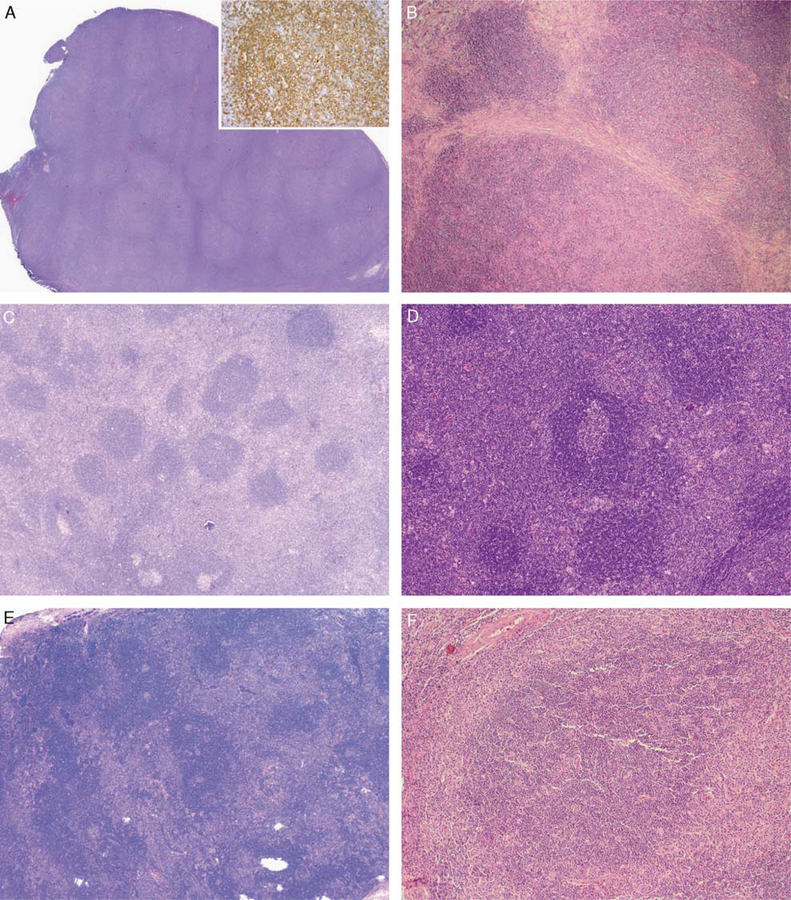
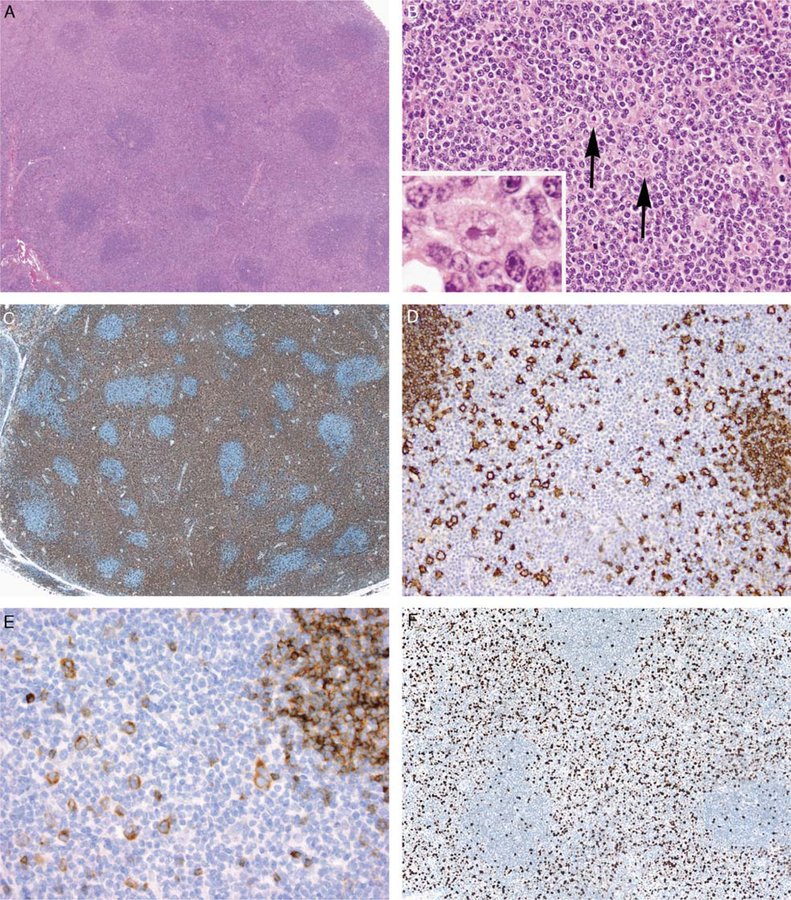
Nodular lymphocyte-predominant Hodgkin lymphoma (NLPHL) is a distinct Hodgkin lymphoma subtype composed of few neoplastic lymphocyte-predominant (LP) cells in a background of reactive small B and T cells. We have seen occasional NLPHL cases that contain background T cells with prominent cytologic atypia, raising the differential diagnosis of peripheral T-cell lymphoma not otherwise specified (PTCL-NOS) or a composite lymphoma. We sought to characterize the clinicopathologic features of such cases. Eleven NLPHL cases with atypical T cells diagnosed from 1977 to 2010 were identified at 2 institutions and compared with 24 control NLPHL cases lacking atypical T cells. All 9 male patients and 2 female patients presented with localized peripheral lymphadenopathy. In comparison with control patients, they were younger (median age, 13.8 vs. 36.1 y; P=0.015), with more frequent cervical lymph node involvement (54.5% vs. 8.3%, P=0.015). In all 11 cases, areas of NLPHL with typical B-cell-rich nodules containing LP cells were present. Nine cases contained sheets of atypical T cells surrounding primary and secondary follicles in a pattern mimicking the T-zone pattern of PTCL-NOS; the remaining 2 cases contained atypical T cells presented as large clusters at the periphery of B-cell-rich nodules. In all cases, the atypical T-cell-rich areas contained rare scattered LP cells, which were IgD in 5 of 7 cases (71.4%). The atypical T cells showed no pan-T-cell antigen loss or aberrant T-cell antigen expression in any case, and polymerase chain reaction or Southern blot analysis showed no evidence of T-cell clonality in 6 cases tested. The atypical T cells exhibited a variable immunophenotype with respect to germinal center, follicular T-helper, T-regulatory, and cytotoxic T-cell markers. Among 8 patients with clinical follow-up (median follow-up: 6.4 y), 5 patients had recurrent NLPHL at 6 months to 12 years after diagnosis and 6 patients are alive without disease at 9 months to 18 years after diagnosis. In comparison with control patients, NLPHL patients with atypical T cells were more likely to develop recurrent NLPHL (71.4% vs. 13.6%, P=0.008) and to have a shorter time to relapse (P=0.04). Our findings suggest that some cases of NLPHL, occurring predominantly in younger patients, contain prominent populations of morphologically atypical T cells that may raise the possibility of concurrent nodal involvement by PTCL-NOS, a rare diagnosis in children. The clinical behavior of these cases appears similar to that of NLPHL with T-cell-rich diffuse areas, with a higher risk of disease recurrence and no difference in overall survival; however, this finding warrants confirmation in studies of larger numbers of patients.
Conflict of interest statement
Conflicts of Interest and Source of Funding: The authors have disclosed that they have no significant relationships with, or financial interest in, any commercial companies pertaining to this article.
Figures
References
-
- Alvaro T, Lejeune M, Salvado MT, et al. Outcome in Hodgkin’s lymphoma can be predicted from the presence of accompanying cytotoxic and regulatory T cells. Clin Cancer Res 2005;11: 1467–1473. - PubMed
-
- Atayar C, Poppema S, Visser L, et al. Cytokine gene expression profile distinguishes CD4+/CD57+ T cells of the nodular lymphocyte predominance type of Hodgkin’s lymphoma from their tonsillar counterparts. J Pathol 2006;208:423–430. - PubMed
-
- Bakshi N, Aljabry M, Akhter S, et al. Tumor microenvironment in nodular lymphocyte predominant Hodgkin lymphoma (NLPHL) influences occurrence of relapses and progression to large cell lymphoma (abstract). Blood 2010;116:2684.
-
- Bennett MH, MacLennan KA, Vaughan Hudson G, et al. Non-Hodgkin’s lymphoma arising in patients treated for Hodgkin’s disease in the BNLI: a 20-year experience. British National Lymphoma Investigation. Ann Oncol 1991;2(Suppl 2):83–92. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
