

Succinate dehydrogenase-deficient GISTs: a clinicopathologic, immunohistochemical, and molecular genetic study of 66 gastric GISTs with predilection to young age
- PMID: 21997692
- PMCID: PMC3193596
- DOI: 10.1097/PAS.0b013e3182260752
Succinate dehydrogenase-deficient GISTs: a clinicopathologic, immunohistochemical, and molecular genetic study of 66 gastric GISTs with predilection to young age
Abstract
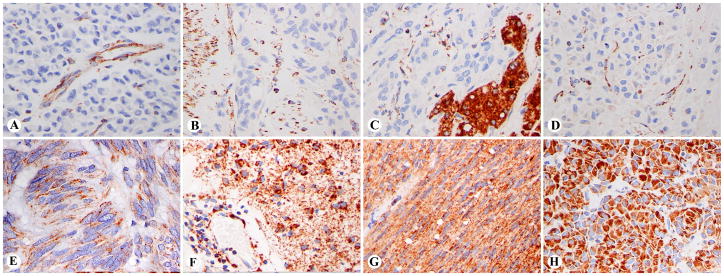
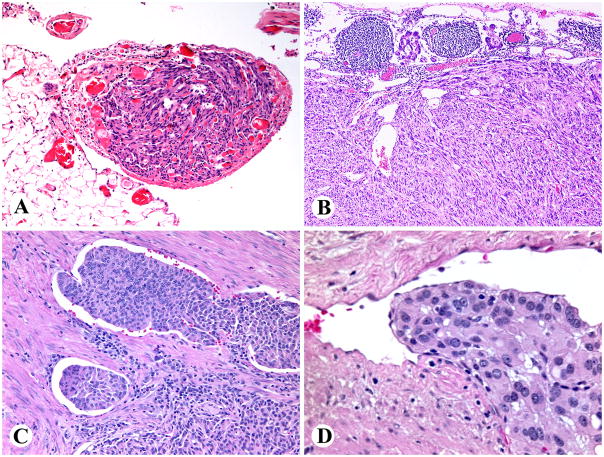
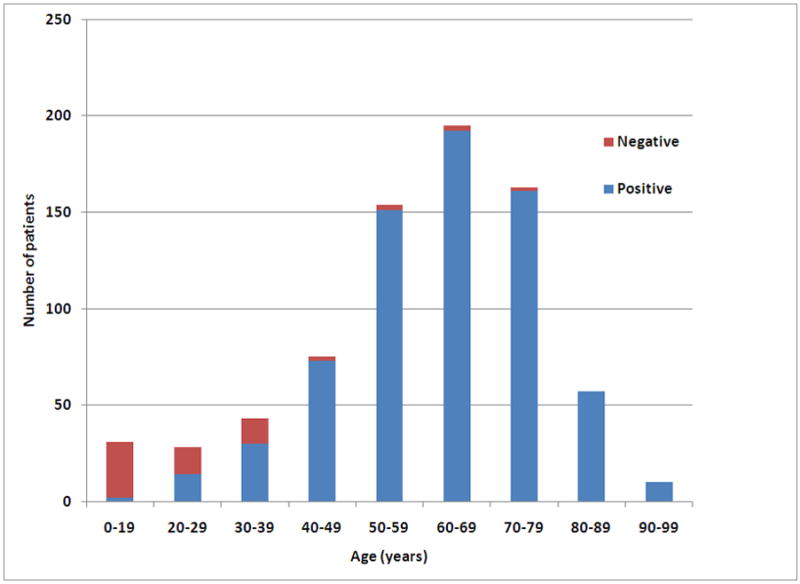
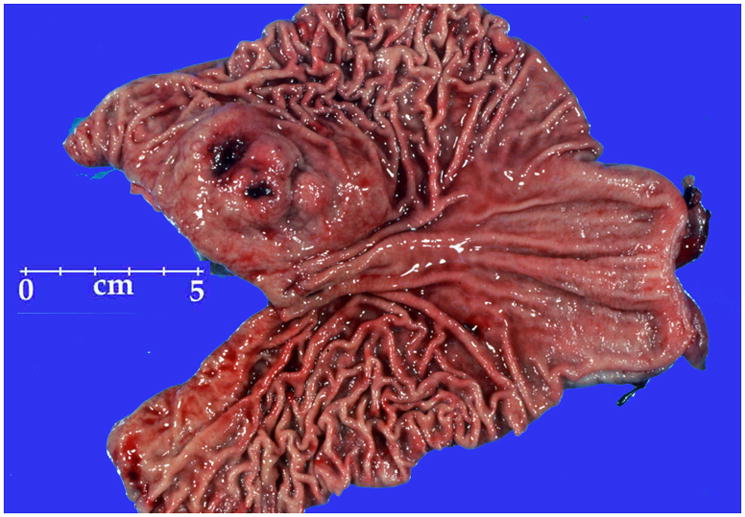
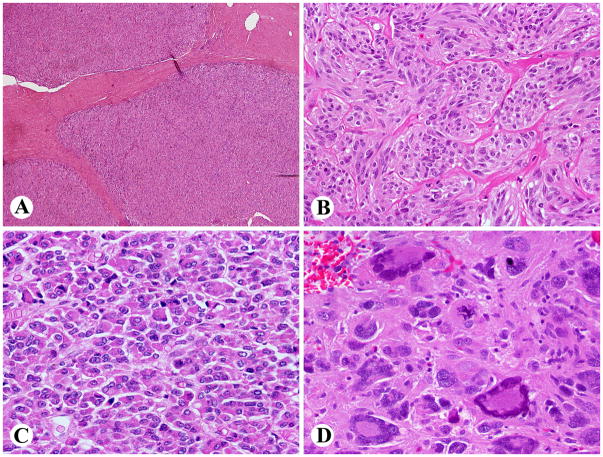
Most gastrointestinal stromal tumors (GISTs) are driven by KIT or PDGFRA-activating mutations, but a small subset is associated with loss of function of the succinate dehydrogenase (SDH) complex of mitochondrial inner membrane proteins. This occurs by germline mutations of the SDH subunit genes and hitherto unknown mechanisms. SDH-deficient GISTs especially include pediatric GISTs and those associated with Carney triad (CT) or Carney-Stratakis syndromes (CSSs); the latter 2 also include paraganglioma as a component. SDH-deficient GISTs were identified in this study on the basis of immunohistochemical loss of succinate dehydrogenase subunit B (SDHB), which signals functional loss of the SDH complex. We found 66 SDH-deficient GISTs among 756 gastric GISTs, with an estimated frequency of 7.5% of unselected cases. Nearly, all gastric GISTs in patients <20 years, and a substantial percentage of those in patients <40 years, but only rare GISTs in older adults were SDH deficient. There was a female predominance of over 2:1. Two patients each had either pulmonary chondroma or paraganglioma (CT), but none of the examined cases had SDH germline mutations (CSS) or somatic KIT/PDGFRA or BRAF mutations. SDH-deficient GISTs were often multiple and typically showed plexiform muscularis propria involvement and epithelioid hypercellular morphology. They were consistently KIT-positive and DOG1/Ano 1-positive and almost always smooth muscle actin negative. Tumor size and mitotic activity varied, and the tumors were somewhat unpredictable with low mitotic rates developing metastases. Gastric recurrences occurred in 11 patients, and peritoneal and liver metastases occurred in 8 and 10 patients, respectively. Lymph node metastases were detected in 5 patients, but lymphovascular invasion was present in >50% of cases studied; these 2 were not related to adverse outcome. Seven patients died of disease, but many had long survivals, even with peritoneal or liver metastases. All 378 nongastric GISTs and 34 gastric non-GIST mesenchymal tumors were SDHB positive. SDH-deficient GISTs constitute a small subgroup of gastric GISTs; they usually occur in children and young adults, often have a chronic course similar to that of pediatric and CT GISTs, and have potential association with paraganglioma, necessitating long-term follow-up.
Figures
References
-
- Burnichon N, Rohmer V, Amar L, et al. The succinate dehydrogenase genetic testing in a large prospective series of patients with paragangliomas. J Endocr Clin Metab. 2009;94:2817–2827. - PubMed
-
- Carney JA. Carney triad: a syndrome featuring paraganglionic, adrenocortical, and possibly other endocrine tumors. J Clin Endocr Metab. 2009;94:3656–3662. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
