

Prognostic utility of the breast cancer index and comparison to Adjuvant! Online in a clinical case series of early breast cancer
- PMID: 21999244
- PMCID: PMC3262211
- DOI: 10.1186/bcr3038
Prognostic utility of the breast cancer index and comparison to Adjuvant! Online in a clinical case series of early breast cancer
Abstract
Introduction: Breast Cancer Index (BCI) combines two independent biomarkers, HOXB13:IL17BR (H:I) and the 5-gene molecular grade index (MGI), that assess estrogen-mediated signalling and tumor grade, respectively. BCI stratifies early-stage estrogen-receptor positive (ER+), lymph-node negative (LN-) breast cancer patients into three risk groups and provides a continuous assessment of individual risk of distant recurrence. Objectives of the current study were to validate BCI in a clinical case series and to compare the prognostic utility of BCI and Adjuvant!Online (AO).
Methods: Tumor samples from 265 ER+LN- tamoxifen-treated patients were identified from a single academic institution's cancer research registry. The BCI assay was performed and scores were assigned based on a pre-determined risk model. Risk was assessed by BCI and AO and correlated to clinical outcomes in the patient cohort.
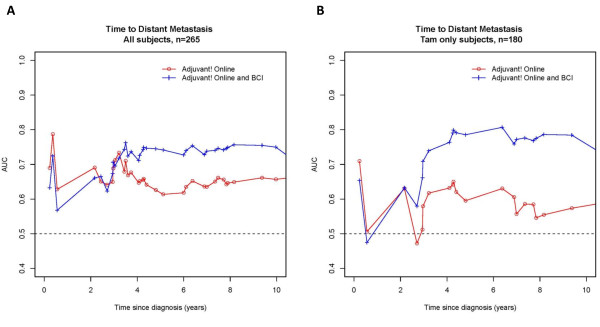
Results: BCI was a significant predictor of outcome in a cohort of 265 ER+LN- patients (median age: 56-y; median follow-up: 10.3-y), treated with adjuvant tamoxifen alone or tamoxifen with chemotherapy (32%). BCI categorized 55%, 21%, and 24% of patients as low, intermediate and high-risk, respectively. The 10-year rates of distant recurrence were 6.6%, 12.1% and 31.9% and of breast cancer-specific mortality were 3.8%, 3.6% and 22.1% in low, intermediate, and high-risk groups, respectively. In a multivariate analysis including clinicopathological factors, BCI was a significant predictor of distant recurrence (HR for 5-unit increase = 5.32 [CI 2.18-13.01; P = 0.0002]) and breast cancer-specific mortality (HR for a 5-unit increase = 9.60 [CI 3.20-28.80; P < 0.0001]). AO was significantly associated with risk of recurrence. In a separate multivariate analysis, both BCI and AO were significantly predictive of outcome. In a time-dependent (10-y) ROC curve accuracy analysis of recurrence risk, the addition of BCI+AO increased predictive accuracy in all patients from 66% (AO only) to 76% (AO+BCI) and in tamoxifen-only treated patients from 65% to 81%.
Conclusions: This study validates the prognostic performance of BCI in ER+LN- patients. In this characteristically low-risk cohort, BCI classified high versus low-risk groups with ~5-fold difference in 10-year risk of distant recurrence and breast cancer-specific death. BCI and AO are independent predictors with BCI having additive utility beyond standard of care parameters that are encompassed in AO.
Figures
References
-
- Fisher B, Jeong JH, Bryant J, Anderson S, Dignam J, Fisher ER, Wolmark N. Treatment of lymph-node-negative, oestrogen-receptor-positive breast cancer: long-term findings from National Surgical Adjuvant Breast and Bowel Project randomised clinical trials. Lancet. 2004;364:858–868. doi: 10.1016/S0140-6736(04)16981-X. - DOI - PubMed
-
- Olivotto IA, Bajdik CD, Ravdin PM, Speers CH, Coldman AJ, Norris BD, Davis GJ, Chia SK, Gelmon KA. Population-based validation of the prognostic model ADJUVANT! for early breast cancer. J Clin Oncol. 2005;23:2716–2725. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
