

A novel technique for fetal heart rate estimation from Doppler ultrasound signal
- PMID: 21999764
- PMCID: PMC3305903
- DOI: 10.1186/1475-925X-10-92
A novel technique for fetal heart rate estimation from Doppler ultrasound signal
Abstract
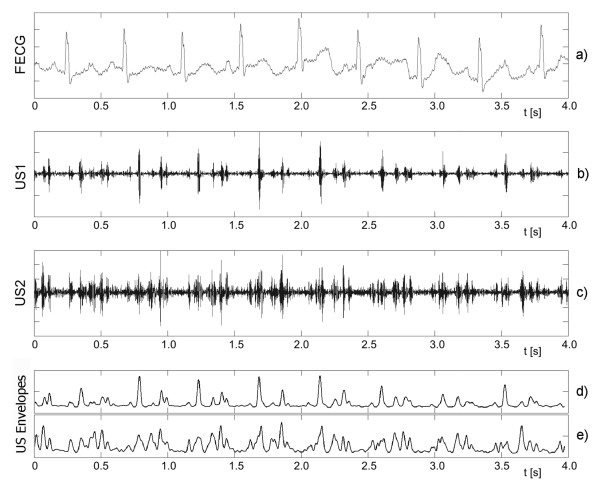
Background: The currently used fetal monitoring instrumentation that is based on Doppler ultrasound technique provides the fetal heart rate (FHR) signal with limited accuracy. It is particularly noticeable as significant decrease of clinically important feature - the variability of FHR signal. The aim of our work was to develop a novel efficient technique for processing of the ultrasound signal, which could estimate the cardiac cycle duration with accuracy comparable to a direct electrocardiography.
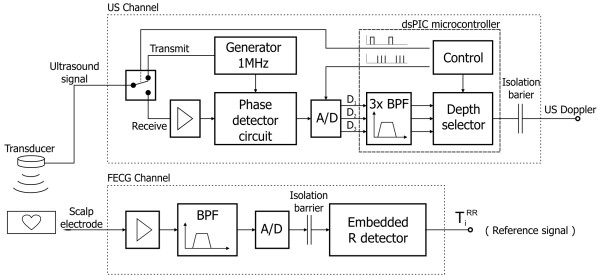
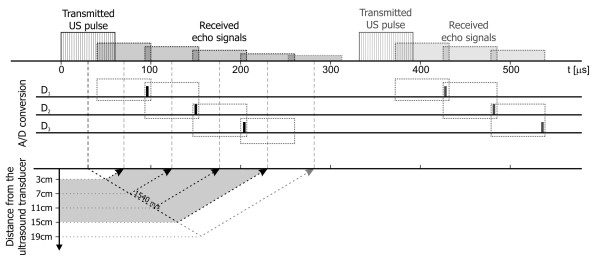
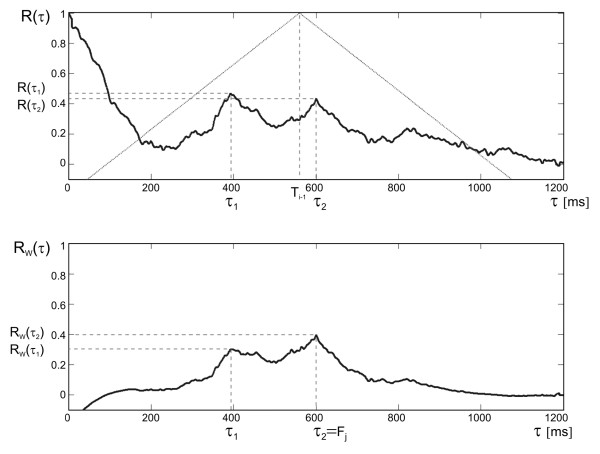
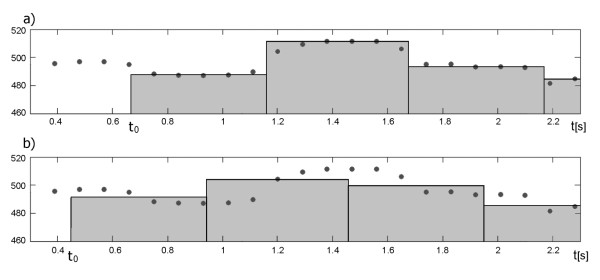
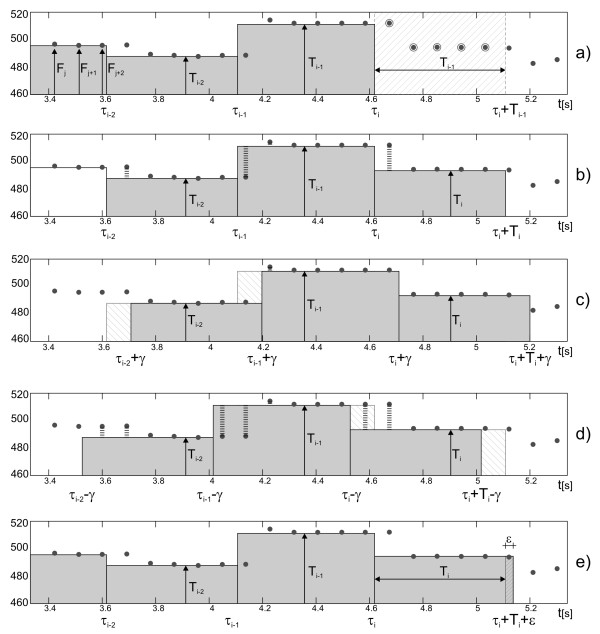
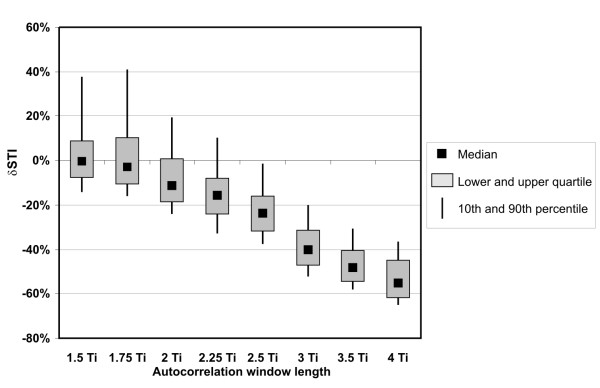
Methods: We have proposed a new technique which provides the true beat-to-beat values of the FHR signal through multiple measurement of a given cardiac cycle in the ultrasound signal. The method consists in three steps: the dynamic adjustment of autocorrelation window, the adaptive autocorrelation peak detection and determination of beat-to-beat intervals. The estimated fetal heart rate values and calculated indices describing variability of FHR, were compared to the reference data obtained from the direct fetal electrocardiogram, as well as to another method for FHR estimation.
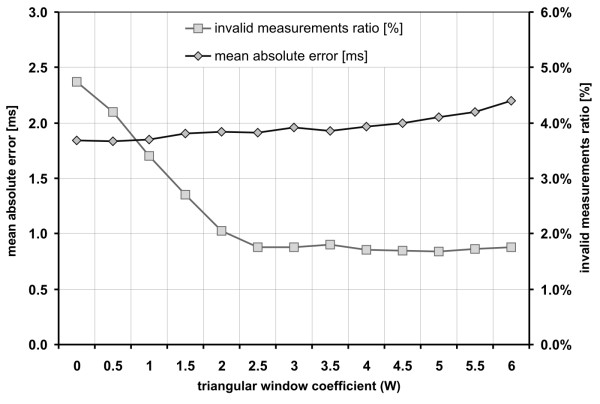
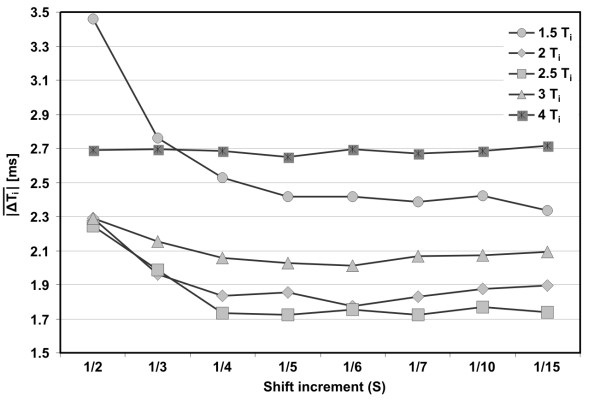
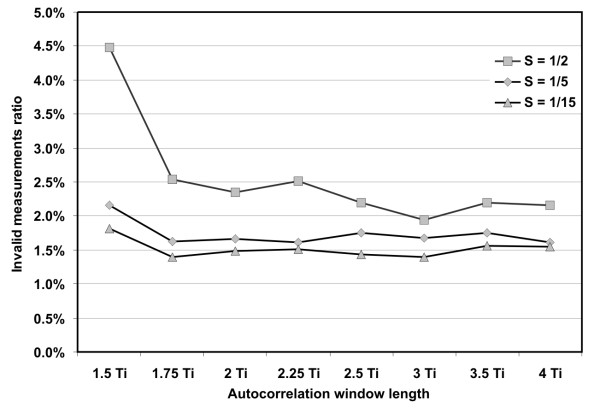
Results: The results revealed that our method increases the accuracy in comparison to currently used fetal monitoring instrumentation, and thus enables to calculate reliable parameters describing the variability of FHR. Relating these results to the other method for FHR estimation we showed that in our approach a much lower number of measured cardiac cycles was rejected as being invalid.
Conclusions: The proposed method for fetal heart rate determination on a beat-to-beat basis offers a high accuracy of the heart interval measurement enabling reliable quantitative assessment of the FHR variability, at the same time reducing the number of invalid cardiac cycle measurements.
Figures

References
-
- Jezewski J, Wrobel J, Horoba K, Cholewa D, Gacek A, Kupka T, Matonia A. Monitoring of mechanical and electrical activity of fetal heart: The nature of signals. Arch Perinat Med. 2002;8:40–46.
-
- Matonia A, Jezewski J, Kupka T, Wrobel J, Horoba K, Widera M. Instrumentation for fetal cardiac performance analysis during the antepartum period. Conf Proc IEEE Eng Med Biol Soc. 2005;27:6675–6678. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
