

The protective role of laparoscopic antireflux surgery against aspiration of pepsin after lung transplantation
- PMID: 22000170
- PMCID: PMC3694415
- DOI: 10.1016/j.surg.2011.07.053
The protective role of laparoscopic antireflux surgery against aspiration of pepsin after lung transplantation
Abstract
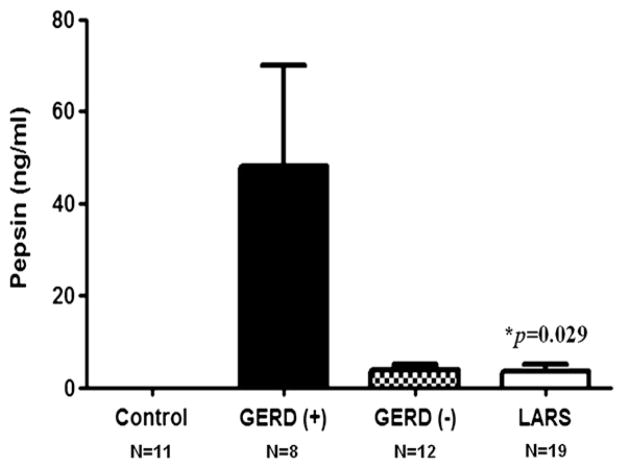
Background: The goal of this study was to determine, in lung transplant patients, if laparoscopic antireflux surgery (LARS) is an effective means to prevent aspiration as defined by the presence of pepsin in the bronchoalveolar lavage fluid (BALF).
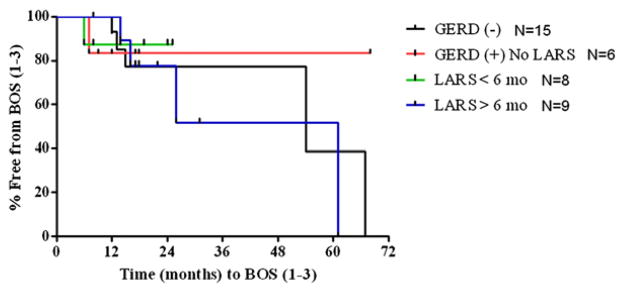
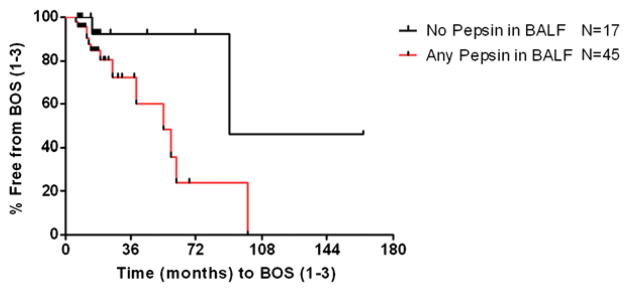
Methods: Between September 2009 and November 2010, we collected BALF from 64 lung transplant patients at multiple routine surveillance assessments for acute cellular rejection, or when clinically indicated for diagnostic purposes. The BALF was tested for pepsin by enzyme-linked immunosorbent assay (ELISA). We then compared pepsin concentrations in the BALF of healthy controls (n = 11) and lung transplant patients with and without gastroesophageal reflux disease (GERD) on pH-monitoring (n = 8 and n = 12, respectively), and after treatment of GERD by LARS (n = 19). Time to the development of bronchiolitis obliterans syndrome was contrasted between groups based on GERD status or the presence of pepsin in the BALF.
Results: We found that lung transplant patients with GERD had more pepsin in their BALF than lung transplant patients who underwent LARS (P = .029), and that pepsin was undetectable in the BALF of controls. Moreover, those with more pepsin had quicker progression to BOS and more acute rejection episodes.
Conclusion: This study compared pepsin in the BALF from lung transplant patients with and without LARS. Our data show that: (1) the detection of pepsin in the BALF proves aspiration because it is not present in healthy volunteers, and (2) LARS appears effective as a measure to prevent the aspiration of gastroesophageal refluxate in the lung transplant population. We believe that these findings provide a mechanism for those studies suggesting that LARS may prevent nonallogenic injury to the transplanted lungs from aspiration of gastroesophageal contents.
Copyright © 2011 Mosby, Inc. All rights reserved.
Figures
Similar articles
-
Pepsin concentrations are elevated in the bronchoalveolar lavage fluid of patients with idiopathic pulmonary fibrosis after lung transplantation.J Surg Res. 2013 Dec;185(2):e101-8. doi: 10.1016/j.jss.2013.06.011. Epub 2013 Jun 29. J Surg Res. 2013. PMID: 23845868 Free PMC article.
-
The diagnostic value of gastroesophageal reflux disease (GERD) symptoms and detection of pepsin and bile acids in bronchoalveolar lavage fluid and exhaled breath condensate for identifying lung transplantation patients with GERD-induced aspiration.Surg Endosc. 2014 Jun;28(6):1794-800. doi: 10.1007/s00464-013-3388-3. Epub 2014 Jan 11. Surg Endosc. 2014. PMID: 24414458 Free PMC article.
-
Pulmonary immune changes early after laparoscopic antireflux surgery in lung transplant patients with gastroesophageal reflux disease.J Surg Res. 2012 Oct;177(2):e65-73. doi: 10.1016/j.jss.2012.03.066. Epub 2012 Apr 18. J Surg Res. 2012. PMID: 22537841 Free PMC article.
-
A review of the potential applications and controversies of non-invasive testing for biomarkers of aspiration in the lung transplant population.Clin Transplant. 2010 May-Jun;24(3):E54-61. doi: 10.1111/j.1399-0012.2010.01243.x. Epub 2010 Mar 19. Clin Transplant. 2010. PMID: 20331688 Free PMC article. Review.
-
Gastroesophageal Reflux Disease and Idiopathic Lung Fibrosis. From Heartburn to Lung Transplant, and Beyond.Am Surg. 2022 Feb;88(2):297-302. doi: 10.1177/0003134821998686. Epub 2021 Feb 25. Am Surg. 2022. PMID: 33629881 Review.
Cited by
-
Developments in lung transplantation over the past decade.Eur Respir Rev. 2020 Jul 21;29(157):190132. doi: 10.1183/16000617.0132-2019. Print 2020 Sep 30. Eur Respir Rev. 2020. PMID: 32699023 Free PMC article. Review.
-
Proton Pump Inhibitors Independently Protect Against Early Allograft Injury or Chronic Rejection After Lung Transplantation.Dig Dis Sci. 2018 Feb;63(2):403-410. doi: 10.1007/s10620-017-4827-0. Epub 2017 Nov 1. Dig Dis Sci. 2018. PMID: 29094310
-
Impaired Esophageal Motility and Clearance Post-Lung Transplant: Risk For Chronic Allograft Failure.Clin Transl Gastroenterol. 2017 Jun 29;8(6):e102. doi: 10.1038/ctg.2017.30. Clin Transl Gastroenterol. 2017. PMID: 28662022 Free PMC article.
-
Antireflux surgery for prevention of chronic lung allograft dysfunction (CLAD) onset after lung transplantation: The earlier the better before CLAD onset? A single-center series of 284 patients.JHLT Open. 2024 Aug 8;6:100145. doi: 10.1016/j.jhlto.2024.100145. eCollection 2024 Nov. JHLT Open. 2024. PMID: 40145037 Free PMC article.
-
LAPAROSCOPIC ANTIREFLUX SURGERY: ARE OLD QUESTIONS ANSWERED? USEFUL FOR EXTRA-ESOPHAGEAL SYMPTOMS?Arq Bras Cir Dig. 2022 Jan 31;34(4):e1632. doi: 10.1590/0102-672020210002e1632. eCollection 2022. Arq Bras Cir Dig. 2022. PMID: 35107494 Free PMC article.
References
-
- Christie JD, Edwards LB, Aurora P, Dobbels F, Kirk R, Rahmel AO, et al. Registry for the International Society for Heart and Lung Transplantation: twenty-fifth Official adult lung and heart/lung transplantation report–2008. J Heart Lung Transplant. 2008;27:957–69. - PubMed
-
- Estenne M, Maurer JR, Boehler A, Egan JJ, Frost A, Hertz M, et al. Bronchiolitis obliterans syndrome 2001: an update of the diagnostic criteria. J Heart Lung Transplant. 2002;21:297–310. - PubMed
-
- D’Ovidio F, Mura M, Tsang M, Waddell TK, Hutcheon MA, Singer LG, et al. Bile acid aspiration and the development of bronchiolitis obliterans after lung transplantation. J Thorac Cardiovasc Surg. 2005;129:1144–52. - PubMed
-
- Hadjiliadis D, Duane Davis R, Steele MP, Messier RH, Lau CL, Eubanks SS, et al. Gastroesophageal reflux disease in lung transplant recipients. Clin Transplant. 2003;17:363–8. - PubMed
-
- Lau CL, Palmer SM, Howell DN, McMahon R, Hadjiliadis D, Gaca J, et al. Laparoscopic antireflux surgery in the lung transplant population. Surg Endosc. 2002;16:1674–8. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
