

Use of the Frank-Starling mechanism during exercise is linked to exercise-induced changes in arterial load
- PMID: 22003052
- PMCID: PMC3334246
- DOI: 10.1152/ajpheart.00147.2011
Use of the Frank-Starling mechanism during exercise is linked to exercise-induced changes in arterial load
Abstract
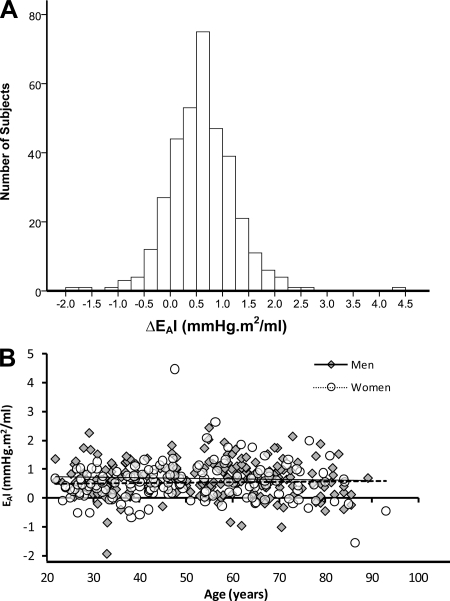
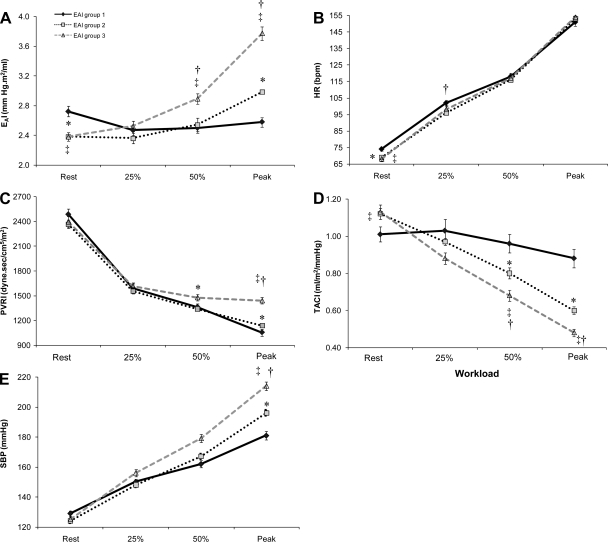
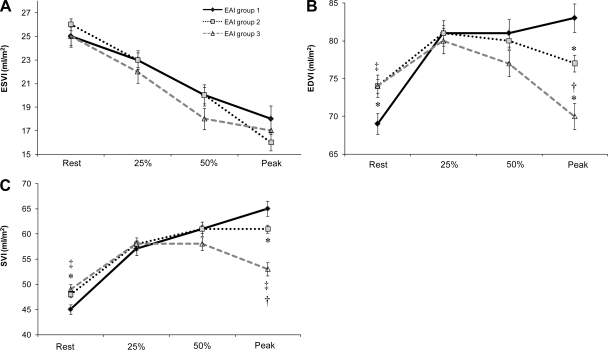
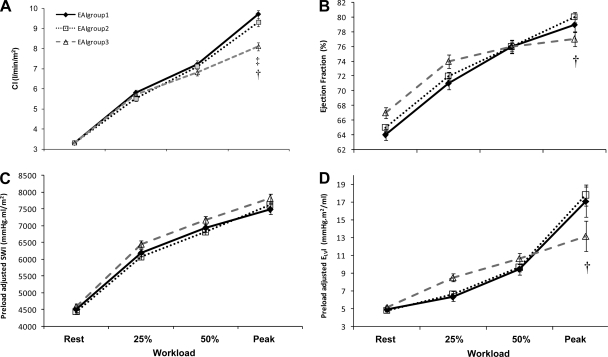
Effective arterial elastance(E(A)) is a measure of the net arterial load imposed on the heart that integrates the effects of heart rate(HR), peripheral vascular resistance(PVR), and total arterial compliance(TAC) and is a modulator of cardiac performance. To what extent the change in E(A) during exercise impacts on cardiac performance and aerobic capacity is unknown. We examined E(A) and its relationship with cardiovascular performance in 352 healthy subjects. Subjects underwent rest and exercise gated scans to measure cardiac volumes and to derive E(A)[end-systolic pressure/stroke volume index(SV)], PVR[MAP/(SV*HR)], and TAC(SV/pulse pressure). E(A) varied with exercise intensity: the ΔE(A) between rest and peak exercise along with its determinants, differed among individuals and ranged from -44% to +149%, and was independent of age and sex. Individuals were separated into 3 groups based on their ΔE(A)I. Individuals with the largest increase in ΔE(A)(group 3;ΔE(A)≥0.98 mmHg.m(2)/ml) had the smallest reduction in PVR, the greatest reduction in TAC and a similar increase in HR vs. group 1(ΔE(A)<0.22 mmHg.m(2)/ml). Furthermore, group 3 had a reduction in end-diastolic volume, and a blunted increase in SV(80%), and cardiac output(27%), during exercise vs. group 1. Despite limitations in the Frank-Starling mechanism and cardiac function, peak aerobic capacity did not differ by group because arterial-venous oxygen difference was greater in group 3 vs. 1. Thus the change in arterial load during exercise has important effects on the Frank-Starling mechanism and cardiac performance but not on exercise capacity. These findings provide interesting insights into the dynamic cardiovascular alterations during exercise.
Figures
Similar articles
-
The impact of 2 years of high-intensity exercise training on a model of integrated cardiovascular regulation.J Physiol. 2019 Jan;597(2):419-429. doi: 10.1113/JP276676. Epub 2018 Nov 22. J Physiol. 2019. PMID: 30387144 Free PMC article. Clinical Trial.
-
Healthy Aging and Cardiovascular Function: Invasive Hemodynamics During Rest and Exercise in 104 Healthy Volunteers.JACC Heart Fail. 2020 Feb;8(2):111-121. doi: 10.1016/j.jchf.2019.08.020. Epub 2019 Nov 6. JACC Heart Fail. 2020. PMID: 31706837 Free PMC article.
-
Vascular-ventricular coupling during exercise is not affected by exaggerated blood pressures in endurance-trained athletes.J Appl Physiol (1985). 2019 Sep 1;127(3):753-759. doi: 10.1152/japplphysiol.00108.2019. Epub 2019 Jul 18. J Appl Physiol (1985). 2019. PMID: 31318617
-
[Value of training-induced effects on arterial vascular system and skeletal muscles in therapy of NYHA II/III heart failure].Z Kardiol. 2001 Nov;90(11):813-23. doi: 10.1007/s003920170080. Z Kardiol. 2001. PMID: 11771449 Review. German.
-
Arterial-ventricular coupling: mechanistic insights into cardiovascular performance at rest and during exercise.J Appl Physiol (1985). 2008 Oct;105(4):1342-51. doi: 10.1152/japplphysiol.90600.2008. Epub 2008 Jul 10. J Appl Physiol (1985). 2008. PMID: 18617626 Free PMC article. Review.
Cited by
-
Gender differences in myocardial function and arterio-ventricular coupling in response to maximal exercise in adolescent floor-ball players.BMC Sports Sci Med Rehabil. 2014 Jun 24;6:24. doi: 10.1186/2052-1847-6-24. eCollection 2014. BMC Sports Sci Med Rehabil. 2014. PMID: 25045524 Free PMC article.
-
Impact of chronic changes in arterial compliance and resistance on left ventricular ageing in humans.Eur J Heart Fail. 2015 Jan;17(1):27-34. doi: 10.1002/ejhf.190. Epub 2014 Oct 31. Eur J Heart Fail. 2015. PMID: 25359272 Free PMC article.
-
Ventricular-Arterial Coupling in Breast Cancer Patients After Treatment With Anthracycline-Containing Adjuvant Chemotherapy.Oncologist. 2016 Feb;21(2):141-9. doi: 10.1634/theoncologist.2015-0352. Epub 2016 Jan 13. Oncologist. 2016. PMID: 26764251 Free PMC article.
-
Isolated neonatal rat papillary muscles: a new model to translate neonatal rat myocyte signaling into contractile mechanics.Physiol Rep. 2016 Feb;4(3):e12694. doi: 10.14814/phy2.12694. Physiol Rep. 2016. PMID: 26869681 Free PMC article.
-
Validity of predicting left ventricular end systolic pressure changes following an acute bout of exercise.J Sci Med Sport. 2013 Jan;16(1):71-5. doi: 10.1016/j.jsams.2012.05.003. Epub 2012 Jun 20. J Sci Med Sport. 2013. PMID: 22721862 Free PMC article.
References
-
- Arbab-Zadeh A, Dijk E, Prasad A, Fu Q, Torres P, Zhang R, Thomas JD, Palmer D, Levine BD. Effect of Aging and Physical Activity on Left Ventricular Compliance. Circulation 110: 1799–1805, 2004 - PubMed
-
- Armentano RL, Levenson J, Barra JG, Fischer EI, Breitbart GJ, Pichel RH, Simon A. Assessment of elastin and collagen contribution to aortic elasticity in conscious dogs. Am J Physiol Heart Circ Physiol 260: H1870–1877, 1991 - PubMed
-
- Asanoi H, Kameyama T, Ishizaka S, Miyagi K, Sasayama S. Ventriculoarterial coupling during exercise in normal human subjects. Int J Cardiol 36: 177–186, 1992 - PubMed
-
- Baicu CF, Zile MR, Aurigemma GP, Gaasch WH. Left Ventricular Systolic Performance, Function, and Contractility in Patients With Diastolic Heart Failure. 111: 2306–2312, 2005 - PubMed
-
- Belcher P, Boerboom LE, Olinger GN. Standardization of end-systolic pressure-volume relation in the dog. Am J Physiol Heart Circ Physiol 249: H547–553, 1985 - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials