

Treating Mycobacterium ulcerans disease (Buruli ulcer): from surgery to antibiotics, is the pill mightier than the knife?
- PMID: 22004037
- PMCID: PMC3243445
- DOI: 10.2217/fmb.11.101
Treating Mycobacterium ulcerans disease (Buruli ulcer): from surgery to antibiotics, is the pill mightier than the knife?
Abstract
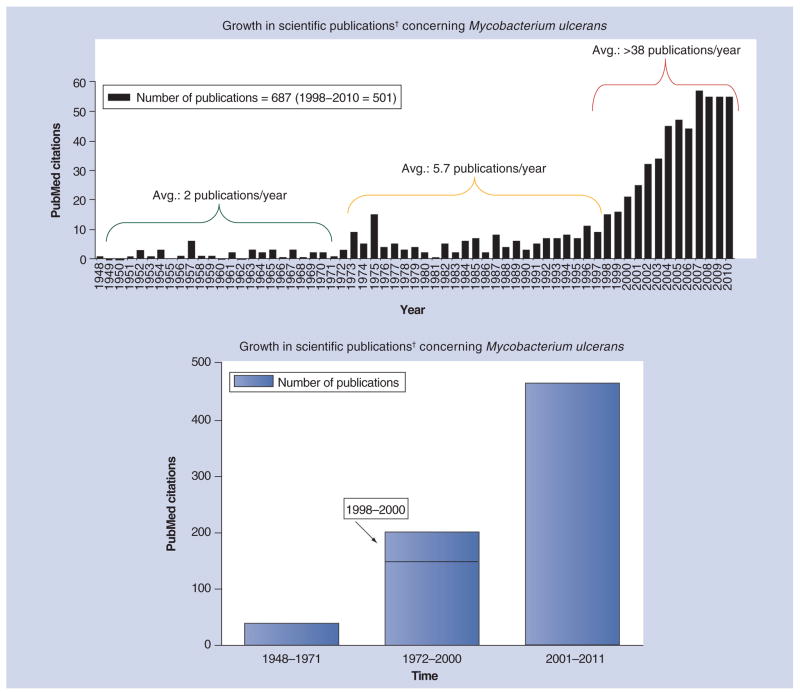
Until 2004, the skin disease known as Buruli ulcer, caused by Mycobacterium ulcerans, could only be treated by surgery and skin grafting. Although this worked reasonably well on early lesions typically found in patients in Australia, the strategy was usually impractical on large lesions resulting from diagnostic delay in patients in rural West Africa. Based on promising preclinical studies, treatment trials in West Africa have shown that a combination of rifampin and streptomycin administered daily for 8 weeks can kill M. ulcerans bacilli, arrest the disease, and promote healing without relapse or reduce the extent of surgical excision. Improved treatment options are the focus of research that has increased tremendously since the WHO began its Global Buruli Ulcer Initiative in 1998.
Figures

References
Bibliography
-
- Lunn HF, Connor DH, Wilks NE, et al. Buruli (mycobacterial) ulceration in Uganda (a new focus of Buruli ulcer in Madi district, Uganda): report of a field study. East Afr Med J. 1965;42:275–288. - PubMed
-
- Stinear T. PhD thesis. Department of Microbiology, Monash University; Clayton, Australia: 2002. Molecular and environmental aspects of Mycobacterium ulcerans.
-
- MacCallum P, Tolhurst JC, Buckle G, Sissons HA. A new mycobacterial infection in man. J Pathol Bacteriol. 1948;60:93–122. - PubMed
-
- Janssens PG, Quertinmont MJ, Sieniawski J, Gatti F. Necrotic tropical ulcers and mycobacterial causative agents. Trop Geogr Med. 1959;11:293–312. - PubMed
-
- Van Oye E, Ballion M. Faudra-t-il tenir compte d’une nouvelle affection à bacilles acido-resistants en Afrique? Note preliminaire. [Is it necessary to take into account a new infection from acid-resistant bacilli in Africa? Preliminary note.] Ann Soc Belg Med Trop. 1950;30(3):619–627. - PubMed
Websites
-
- WHO. WHO joins battle against a new emerging disease, Buruli ulcer. 1997 www.who.int/buruli/information/antibiotics/en/index16.html. - PubMed
-
- WHO. Buruli ulcer. www.who.int/buruli/gbui/en/index.html.
-
- WHO. Geneva: 2004. Provisional guidance on the role of specific antibiotics in the management of Mycobacterium ulcerans disease (Buruli ulcer) www.who.int/buruli/information/antibiotics/en/
-
- WHO. New recording and reporting forms for Buruli ulcer. www.who.int/Buruli/control/forms_2/en.
-
- Bassler BL. How bacteria “talk”. TED Talks. 2009 www.ted.com/talks/bonnie_bassler_on_how_bacteria_communicate.html.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical