

Growth restriction in gastroschisis: quantification of its severity and exploration of a placental cause
- PMID: 22004141
- PMCID: PMC3214135
- DOI: 10.1186/1471-2431-11-90
Growth restriction in gastroschisis: quantification of its severity and exploration of a placental cause
Abstract
Background: Gastroschisis patients are commonly small for gestational age (SGA, birth weight [BW] < 10th centile). However, the extent, symmetry and causes of that growth restriction remain controversial.
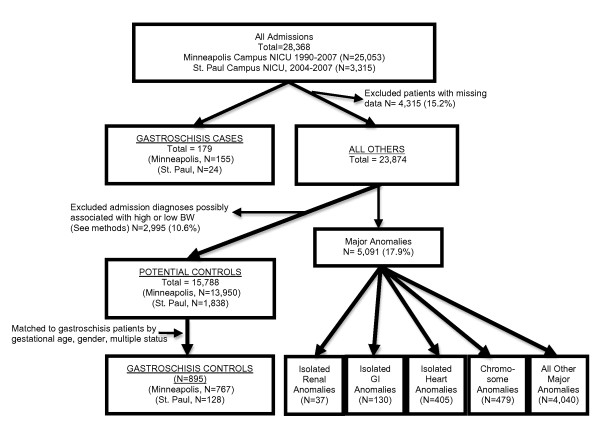
Methods: We compared BW, crown-heel length (LT), occipitofrontal circumference (OFC) and ponderal index (PI) in 179 gastroschisis cases and 895 matched controls by univariate and multiple regression. Fetal ultrasounds (N = 80) were reviewed to determine onset of growth restriction. Placental histology was examined in 31 gastroschisis patients whose placental tissue was available and in 29 controls.
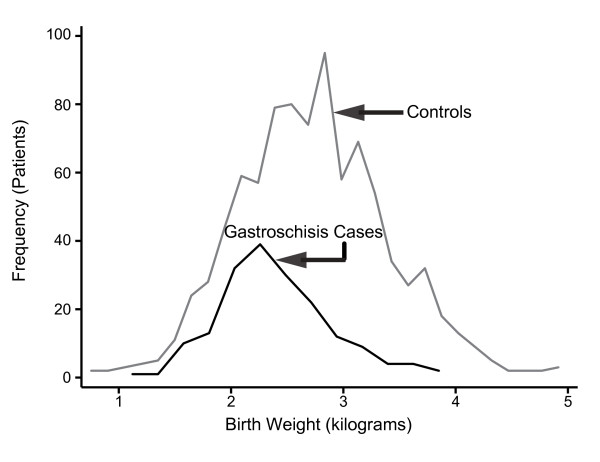
Results: Gastroschisis cases weighed less than controls (BW = 2400 ± 502 g vs. 2750 ± 532 g, p < 0.001) and their BW frequency curve was shifted to the left, indicating lower BW as a group compared to controls (p < 0.001 by Kolmogorov-Smirnov test). BW differences varied from -148 g at 33 weeks to -616 g at 38 weeks gestation. Intrauterine growth restriction was symmetric with gastroschisis patients having a shorter LT (45.7 ± 3.3 vs. 48.4 ± 2.7 cm, p < 0.001), smaller OFC (31.9 ± 1.9 vs. 32.9 ± 1.6 cm, p < 0.001), but larger ponderal index (2.51 ± 0.37 vs. 2.40 ± 0.16, p < 0.001) compared to controls. Gastroschisis patients had a similar reduction in BW (-312 g, 95% confidence interval [CI] = -367, -258) compared to those with chromosomal abnormalities (-239 g, CI = -292, -187). Growth deficits appeared early in the second trimester and worsened as gestation increased. Placental chorangiosis was more common in gastroschisis patients than controls, even after removing all SGA patients (77% vs. 42%, p = 0.02).
Conclusions: Marked, relatively symmetric intrauterine growth restriction is an intrinsic part of gastroschisis. It begins early in the second trimester, and is associated with placental chorangiosis.
Figures





Similar articles
-
Intrauterine growth restriction in infants of less than thirty-two weeks' gestation: associated placental pathologic features.Am J Obstet Gynecol. 1995 Oct;173(4):1049-57. doi: 10.1016/0002-9378(95)91325-4. Am J Obstet Gynecol. 1995. PMID: 7485292
-
Gastroschisis: incidence and prediction of growth restriction.J Perinat Med. 2015 Sep;43(5):605-8. doi: 10.1515/jpm-2014-0283. J Perinat Med. 2015. PMID: 25460279
-
Pregnancy outcome and placental pathology in small for gestational age neonates in relation to the severity of their growth restriction.J Matern Fetal Neonatal Med. 2019 May;32(9):1468-1473. doi: 10.1080/14767058.2017.1408070. Epub 2017 Dec 3. J Matern Fetal Neonatal Med. 2019. PMID: 29157050
-
The significance of intrauterine growth restriction is different from prematurity for the outcome of infants with gastroschisis.J Pediatr Surg. 2004 Aug;39(8):1200-4. doi: 10.1016/j.jpedsurg.2004.04.014. J Pediatr Surg. 2004. PMID: 15300527 Review.
-
Diagnostic performance of third-trimester ultrasound for the prediction of late-onset fetal growth restriction: a systematic review and meta-analysis.Am J Obstet Gynecol. 2019 May;220(5):449-459.e19. doi: 10.1016/j.ajog.2018.09.043. Epub 2019 Jan 8. Am J Obstet Gynecol. 2019. PMID: 30633918
Cited by
-
Growth Failure Prevalence in Neonates with Gastroschisis : A Statewide Cohort Study.J Pediatr. 2021 Jun;233:112-118.e3. doi: 10.1016/j.jpeds.2021.02.013. Epub 2021 Feb 26. J Pediatr. 2021. PMID: 33647253 Free PMC article.
-
A retrospective review of gastroschisis epidemiology and referral patterns in northern Ghana.Pediatr Surg Int. 2021 Aug;37(8):1069-1078. doi: 10.1007/s00383-021-04898-y. Epub 2021 May 31. Pediatr Surg Int. 2021. PMID: 34059928
-
Diverse mechanisms underlying the fetal growth course in gastroschisis and omphalocele.AJOG Glob Rep. 2023 Jun 4;3(3):100238. doi: 10.1016/j.xagr.2023.100238. eCollection 2023 Aug. AJOG Glob Rep. 2023. PMID: 37424955 Free PMC article.
-
A retrospective segmentation analysis of placental volume by magnetic resonance imaging from first trimester to term gestation.Pediatr Radiol. 2018 Dec;48(13):1936-1944. doi: 10.1007/s00247-018-4213-x. Epub 2018 Jul 20. Pediatr Radiol. 2018. PMID: 30027370
-
Longitudinal growth of children born with gastroschisis or omphalocele.Eur J Pediatr. 2023 Dec;182(12):5615-5623. doi: 10.1007/s00431-023-05217-4. Epub 2023 Oct 11. Eur J Pediatr. 2023. PMID: 37819418 Free PMC article.
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
