

Placental Plasmodium falciparum malaria infection: operational accuracy of HRP2 rapid diagnostic tests in a malaria endemic setting
- PMID: 22004666
- PMCID: PMC3206496
- DOI: 10.1186/1475-2875-10-306
Placental Plasmodium falciparum malaria infection: operational accuracy of HRP2 rapid diagnostic tests in a malaria endemic setting
Abstract
Background: Malaria has a negative effect on the outcome of pregnancy. Pregnant women are at high risk of severe malaria and severe haemolytic anaemia, which contribute 60-70% of foetal and perinatal losses. Peripheral blood smear microscopy under-estimates sequestered placental infections, therefore malaria rapid diagnostic tests (RDTs) detecting histidine rich protein-2 antigen (HRP-2) in peripheral blood are a potential alternative.
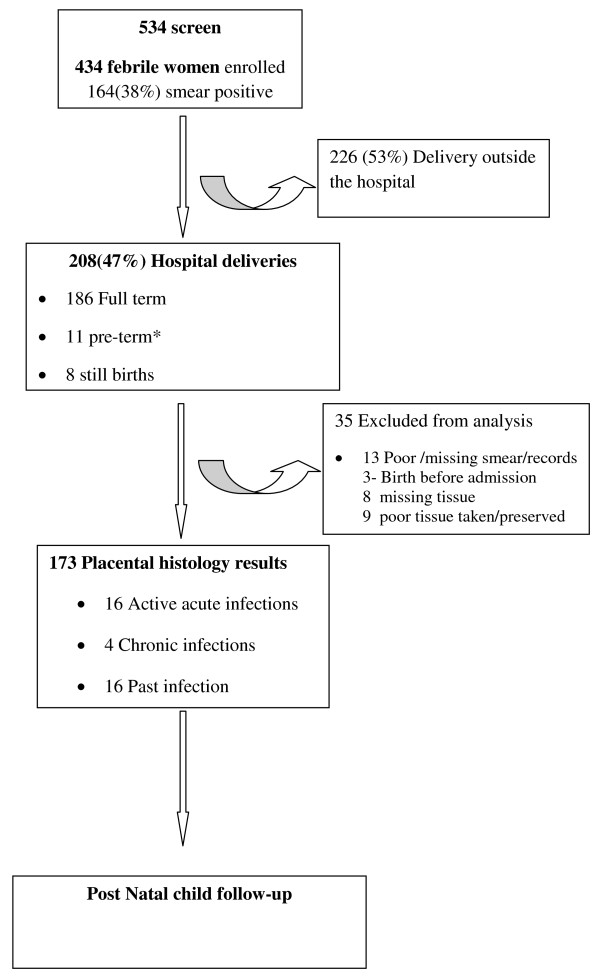
Methods: HRP-2 RDTs accuracy in detecting malaria in pregnancy (MIP >28 weeks gestation) and placental Plasmodium falciparum malaria (after childbirth) were conducted using Giemsa microscopy and placental histopathology respectively as the reference standard. The study was conducted in Mbale Hospital, using the midwives to perform and interpret the RDT results. Discordant results samples were spot checked using PCR techniques.
Results: Among 433 febrile women tested, RDTs had a sensitivity of 96.8% (95% CI 92-98.8), specificity of 73.5% (95% CI 67.8-78.6), a positive predictive value (PPV) of 68.0% (95% CI 61.4-73.9), and negative predictive value (NPV) of 97.5% (95% CI 94.0-99.0) in detecting peripheral P. falciparum malaria during pregnancy. At delivery, in non-symptomatic women, RDTs had a 80.9% sensitivity (95% CI 57.4-93.7) and a 87.5% specificity (95%CI 80.9-92.1), PPV of 47.2% (95% CI 30.7-64.2) and NPV of 97.1% (95% CI 92.2-99.1) in detecting placental P. falciparum infections among 173 samples. At delivery, 41% of peripheral infections were detected by microscopy without concurrent placental infection. The combination of RDTs and microscopy improved the sensitivity to 90.5% and the specificity to 98.4% for detecting placental malaria infection (McNemar's X(2)> 3.84). RDTs were not superior to microscopy in detecting placental infection (McNemar's X(2)< 3.84). Presence of malaria in pregnancy and active placental malaria infection were 38% and 12% respectively. Placental infections were associated with poor pregnancy outcome [pre-term, still birth and low birth weight] (aOR = 37.9) and late pregnancy malaria infection (aOR = 20.9). Mosquito net use (aOR 2.1) and increasing parity (aOR 2.7) were associated with lower risk for malaria in pregnancy.
Conclusion: Use of HRP-2 RDTs to detect malaria in pregnancy in symptomatic women was accurate when performed by midwives. A combination of RDTs and microscopy provided the best means of detecting placental malaria. RDTs were not superior to microscopy in detecting placental infection. With a high sensitivity and specificity, RDTs could be a useful tool for assessing malaria in pregnancy, with further (cost-) effectiveness studies.
Figures
Similar articles
-
Accuracy of an HRP-2/panLDH rapid diagnostic test to detect peripheral and placental Plasmodium falciparum infection in Papua New Guinean women with anaemia or suspected malaria.Malar J. 2015 Oct 19;14:412. doi: 10.1186/s12936-015-0927-5. Malar J. 2015. PMID: 26480941 Free PMC article.
-
Accuracy of One Step malaria rapid diagnostic test (RDT) in detecting Plasmodium falciparum placental malaria infection in women living in Yaoundé, Cameroon.Malar J. 2018 Dec 4;17(1):450. doi: 10.1186/s12936-018-2595-8. Malar J. 2018. PMID: 30514316 Free PMC article.
-
Systematic review and meta-analysis: rapid diagnostic tests versus placental histology, microscopy and PCR for malaria in pregnant women.Malar J. 2011 Oct 28;10:321. doi: 10.1186/1475-2875-10-321. Malar J. 2011. PMID: 22035448 Free PMC article.
-
Operational accuracy and comparative persistent antigenicity of HRP2 rapid diagnostic tests for Plasmodium falciparum malaria in a hyperendemic region of Uganda.Malar J. 2008 Oct 29;7:221. doi: 10.1186/1475-2875-7-221. Malar J. 2008. PMID: 18959777 Free PMC article.
-
Summary of discordant results between rapid diagnosis tests, microscopy, and polymerase chain reaction for detecting Plasmodium mixed infection: a systematic review and meta-analysis.Sci Rep. 2020 Jul 29;10(1):12765. doi: 10.1038/s41598-020-69647-y. Sci Rep. 2020. PMID: 32728145 Free PMC article.
Cited by
-
Clinical signs and symptoms cannot reliably predict Plasmodium falciparum malaria infection in pregnant women living in an area of high seasonal transmission.Malar J. 2013 Dec 27;12:464. doi: 10.1186/1475-2875-12-464. Malar J. 2013. PMID: 24373481 Free PMC article.
-
Accuracy of an HRP-2/panLDH rapid diagnostic test to detect peripheral and placental Plasmodium falciparum infection in Papua New Guinean women with anaemia or suspected malaria.Malar J. 2015 Oct 19;14:412. doi: 10.1186/s12936-015-0927-5. Malar J. 2015. PMID: 26480941 Free PMC article.
-
Factors Affecting the Performance of HRP2-Based Malaria Rapid Diagnostic Tests.Trop Med Infect Dis. 2022 Sep 25;7(10):265. doi: 10.3390/tropicalmed7100265. Trop Med Infect Dis. 2022. PMID: 36288006 Free PMC article. Review.
-
Performance of rapid diagnostic test, light microscopy, and polymerase chain reaction in pregnant women with asymptomatic malaria in Nigeria.IJID Reg. 2024 Aug 2;12:100416. doi: 10.1016/j.ijregi.2024.100416. eCollection 2024 Sep. IJID Reg. 2024. PMID: 39253688 Free PMC article.
-
HRP2 and pLDH-Based Rapid Diagnostic Tests, Expert Microscopy, and PCR for Detection of Malaria Infection during Pregnancy and at Delivery in Areas of Varied Transmission: A Prospective Cohort Study in Burkina Faso and Uganda.PLoS One. 2016 Jul 5;11(7):e0156954. doi: 10.1371/journal.pone.0156954. eCollection 2016. PLoS One. 2016. PMID: 27380525 Free PMC article.
References
-
- van Geertruyden JP, Thomas F, Erhart A, D'Alessandro U. The contribution of malaria in pregnancy to perinatal mortality. Am J Trop Med Hyg. 2004;71:35–40. - PubMed
-
- Adam I. Impact of maternal Plasmodium falciparum malaria and haematological parameters on pregnancy and its outcome in southeastern Nigeria. J Vector Borne Dis. 2008;45:78–79. author reply 79-80. - PubMed
-
- Adebami OJ, Owa JA, Oyedeji GA, Oyelami OA, Omoniyi-Esan GO. Associations between placental and cord blood malaria infection and fetal malnutrition in an area of malaria holoendemicity. Am J Trop Med Hyg. 2007;77:209–213. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
