

Impact of inadequate empirical therapy on the mortality of patients with bloodstream infections: a propensity score-based analysis
- PMID: 22005999
- PMCID: PMC3256027
- DOI: 10.1128/AAC.00462-11
Impact of inadequate empirical therapy on the mortality of patients with bloodstream infections: a propensity score-based analysis
Abstract
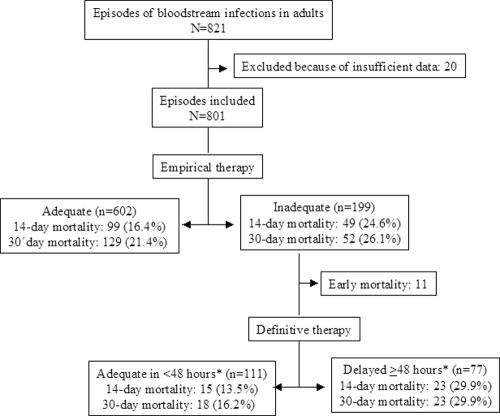
The impact of the adequacy of empirical therapy on outcome for patients with bloodstream infections (BSI) is key for determining whether adequate empirical coverage should be prioritized over other, more conservative approaches. Recent systematic reviews outlined the need for new studies in the field, using improved methodologies. We assessed the impact of inadequate empirical treatment on the mortality of patients with BSI in the present-day context, incorporating recent methodological recommendations. A prospective multicenter cohort including all BSI episodes in adult patients was performed in 15 hospitals in Andalucía, Spain, over a 2-month period in 2006 to 2007. The main outcome variables were 14- and 30-day mortality. Adjusted analyses were performed by multivariate analysis and propensity score-based matching. Eight hundred one episodes were included. Inadequate empirical therapy was administered in 199 (24.8%) episodes; mortality at days 14 and 30 was 18.55% and 22.6%, respectively. After controlling for age, Charlson index, Pitt score, neutropenia, source, etiology, and presentation with severe sepsis or shock, inadequate empirical treatment was associated with increased mortality at days 14 and 30 (odds ratios [ORs], 2.12 and 1.56; 95% confidence intervals [95% CI], 1.34 to 3.34 and 1.01 to 2.40, respectively). The adjusted ORs after a propensity score-based matched analysis were 3.03 and 1.70 (95% CI, 1.60 to 5.74 and 0.98 to 2.98, respectively). In conclusion, inadequate empirical therapy is independently associated with increased mortality in patients with BSI. Programs to improve the quality of empirical therapy in patients with suspicion of BSI and optimization of definitive therapy should be implemented.
Figures
References
-
- Arias CA, Murray BE. 2009. Antibiotic-resistant bugs in the 21st century: a clinical super-challenge. N. Engl. J. Med. 360:439–443 - PubMed
-
- Chang FY, et al. 2003. Staphylococcus aureus bacteremia. Recurrence and the impact of antibiotic treatment in a prospective multicenter study. Medicine (Baltimore, MD) 82:323–329 - PubMed
-
- Charlson ME, Pompei P, Ales KL, MacKenzie CR. 1987. A new method of classifying prognostic co-morbidity in longitudinal studies: development and validation. J. Chronic Dis. 40:373–383 - PubMed
-
- Chow JW, et al. 1991. Enterobacter bacteremia: clinical features and emergence of antibiotic resistance during therapy. Ann. Intern. Med. 115:585–590 - PubMed
-
- Cisneros-Herreros JM, Cobo-Reinoso J, Pujol-Rojo M, Rodríguez-Baño J, Salavert-Lletí M. 2007. Guía para el diagnóstico y tratamiento del paciente con bacteriemia. Guías de la Sociedad Española de Enfermedades Infecciosas y Microbiología Clínica (SEIMC). Enferm. Infecc. Microbiol. Clin. 25:111–130 - PubMed
