

The John Insall Award: no functional advantage of a mobile bearing posterior stabilized TKA
- PMID: 22006197
- PMCID: PMC3238000
- DOI: 10.1007/s11999-011-2114-5
The John Insall Award: no functional advantage of a mobile bearing posterior stabilized TKA
Abstract
Background: Mobile bearing (MB) total knee design has been advocated as a means to enhance the functional characteristics and decrease the wear rates of condylar total knee arthroplasty (TKA). However, it is unclear if these designs achieve these goals.
Questions/purposes: We asked whether function of patients or survivorship would be greater or complications would be lesser in groups of patients with MB compared with fixed bearing (FB) TKA. We also sought to describe retrieval findings.
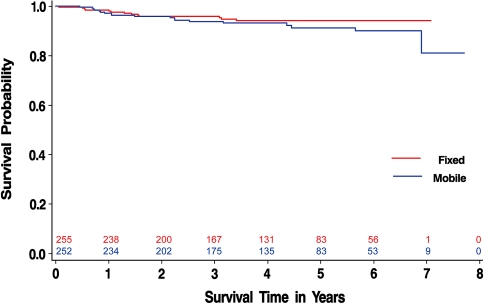
Methods: We randomized 507 primary TKAs in 416 eligible patients to receive MB (n = 252) or FB (n = 255) devices from November 2001 to August 2007 (Investigational Device Exemption G000180, ClinicalTrials.gov registration number NCT00946075). Patients were blinded to treatment allocation. WOMAC Index, SF-12 Health Survey, knee range of motion, and Knee Society scores were collected and compared preoperatively and at 6, 12, and 24 months postoperatively. We recorded device failures and complications until October 2009. Kaplan-Meier survivorship was compared using the log rank test. Twelve retrieved MB devices underwent pathologic analysis. The minimum postoperative time was 2.2 years (mean, 5.9 years; range, 2.2-7.9 years).
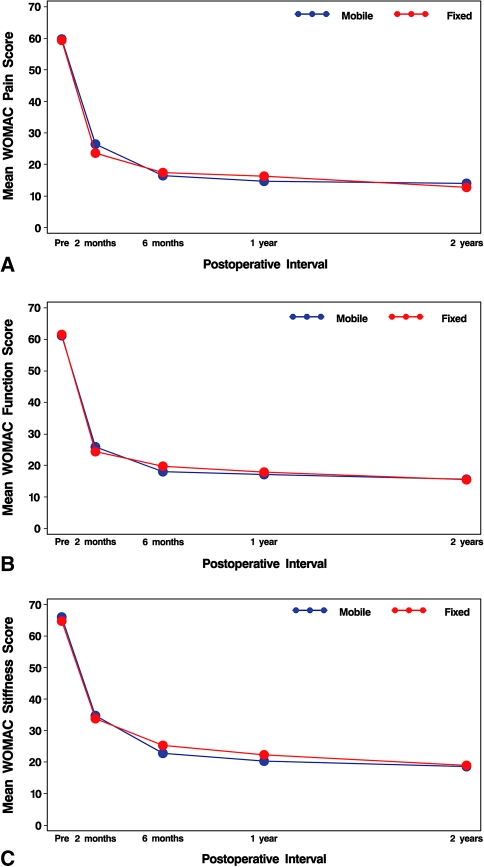
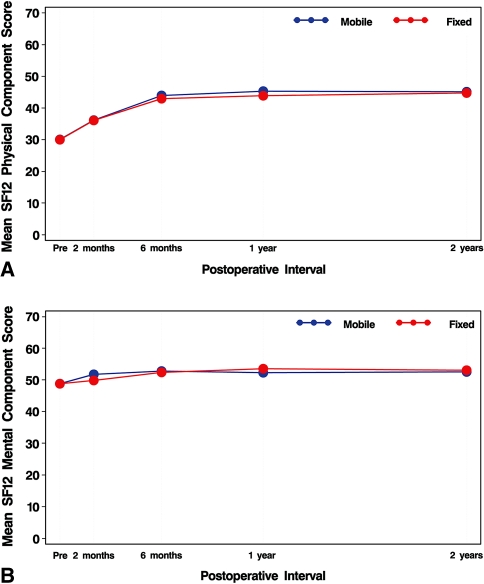
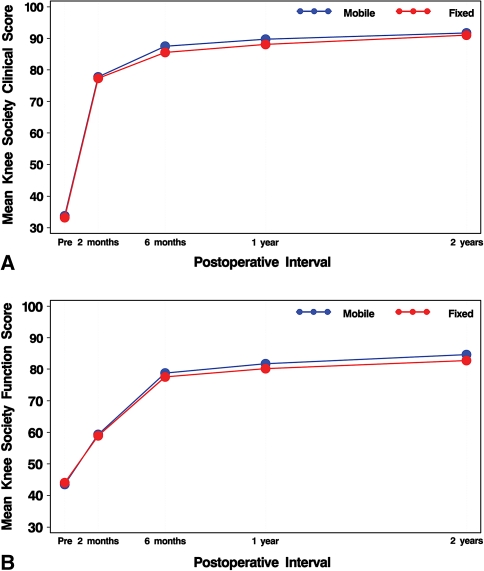
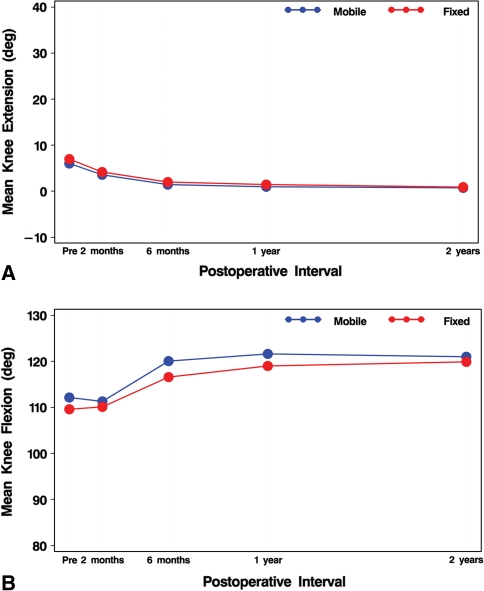
Results: We found no differences in mean clinical assessment scores or mean score changes from baseline at any postoperative interval through 2 postoperative years. Nineteen of the 252 MB and 13 of the 255 FB knees had undergone revision of any component. Estimated survival at 6 postoperative years was similar for the two devices: 90.1% (95% confidence interval [CI], 84.1-93.9) for MB and 94.2% (95% CI, 90.1-96.6) for FB. Two MB and no FB tibial components were revised for loosening. There was one case of MB insert dislocation. Retrieved MB devices demonstrated no unexpected wear or mechanical device failures.
Conclusion: We found no evidence of functional advantage of the MB design. Survivorship was similar, although the study is limited by short duration of followup.
Figures

References
-
- Argenson JN, O’Connor JJ. Polyethylene wear in meniscal knee replacement. A one to nine-year retrieval analysis of the Oxford knee. J Bone Joint Surg Br. 1992;74:228–232. - PubMed
-
- Bellamy N, Buchanan WW, Goldsmith CH, Campbell J, Stitt LW. Validation study of WOMAC: a health status instrument for measuring clinically important patient relevant outcomes to antirheumatic drug therapy in patients with osteoarthritis of the hip or knee. J Rheumatol. 1988;15:1833–1840. - PubMed
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
