

Spread of methicillin-resistant Staphylococcus aureus in a large tertiary NICU: network analysis
- PMID: 22007011
- PMCID: PMC3208963
- DOI: 10.1542/peds.2010-2562
Spread of methicillin-resistant Staphylococcus aureus in a large tertiary NICU: network analysis
Abstract
Objective: Methicillin-resistant Staphylococcus aureus (MRSA) colonization in NICUs increases the risk of nosocomial infection. Network analysis provides tools to examine the interactions among patients and staff members that put patients at risk of colonization.
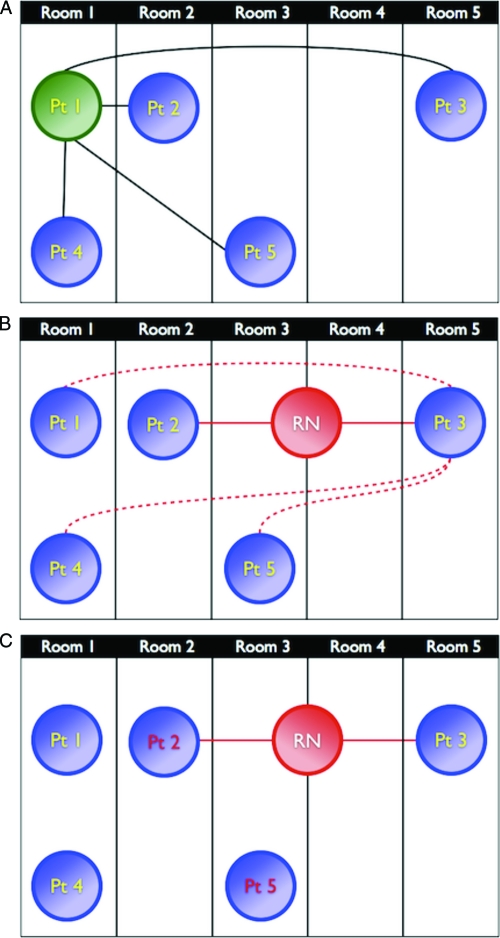
Methods: Data from MRSA surveillance cultures were combined with patient room locations, nursing assignments, and sibship information to create patient- and unit-based networks. Multivariate models were constructed to quantify the risk of incident MRSA colonization as a function of exposure to MRSA-colonized infants in these networks.
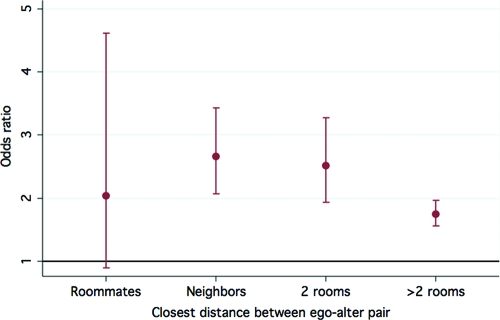
Results: A MRSA-negative infant in the NICU simultaneously with a MRSA-positive infant had higher odds of becoming colonized when the colonized infant was a sibling, compared with an unrelated patient (odds ratio: 8.8 [95% confidence interval [CI]: 5.3-14.8]). Although knowing that a patient was MRSA-positive and was placed on contact precautions reduced the overall odds of another patient becoming colonized by 35% (95% CI: 20%-47%), having a nurse in common with that patient still increased the odds of colonization by 43% (95% CI: 14%-80%). Normalized group degree centrality, a unitwide network measure of connectedness between colonized and uncolonized patients, was a significant predictor of incident MRSA cases (odds ratio: 18.1 [95% CI: 3.6-90.0]).
Conclusions: Despite current infection-control strategies, patients remain at significant risk of MRSA colonization from MRSA-positive siblings and from other patients with whom they share nursing care. Strategies that minimize the frequency of staff members caring for both colonized and uncolonized infants may be beneficial in reducing the spread of MRSA colonization.
Figures
References
-
- Carey AJ, Duchon J, Della-Latta P, Saiman L. The epidemiology of methicillin-susceptible and methicillin-resistant Staphylococcus aureus in a neonatal intensive care unit, 2000–2007. J Perinatol. 2010;30(2):135–139 - PubMed
-
- Gerber SI, Jones RC, Scott MV, et al. Management of outbreaks of methicillin-resistant Staphylococcus aureus infection in the neonatal intensive care unit: a consensus statement. Infect Control Hosp Epidemiol. 2006;27(2):139–145 - PubMed
-
- Gregory ML, Eichenwald EC, Puopolo KM. Seven-year experience with a surveillance program to reduce methicillin-resistant Staphylococcus aureus colonization in a neonatal intensive care unit. Pediatrics. 2009;123(5). Available at: www.pediatrics.org/cgi/content/full/123/5/e790 - PubMed
-
- Back NA, Linnemann CC, Jr, Staneck JL, Kotagal UR. Control of methicillin-resistant Staphylococcus aureus in a neonatal intensive-care unit: use of intensive microbiologic surveillance and mupirocin. Infect Control Hosp Epidemiol. 1996;17(4):227–231 - PubMed
-
- Jernigan JA, Titus MG, Gröschel DH, Getchell-White S, Farr BM. Effectiveness of contact isolation during a hospital outbreak of methicillin-resistant Staphylococcus aureus. Am J Epidemiol. 1996;143(5):496–504 - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
