

Assessment of stromal invasion for correct histological diagnosis of early hepatocellular carcinoma
- PMID: 22007311
- PMCID: PMC3170744
- DOI: 10.4061/2011/241652
Assessment of stromal invasion for correct histological diagnosis of early hepatocellular carcinoma
Abstract
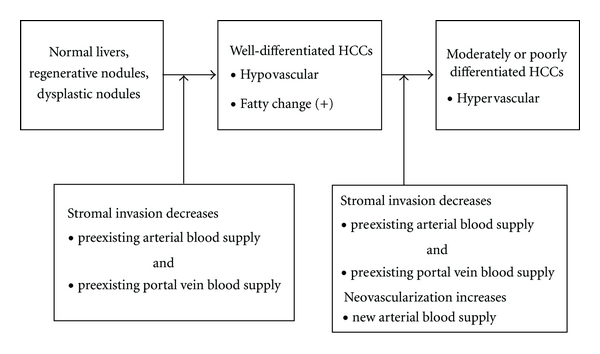
Stromal invasion (invasive growth of tumor tissue into portal tracts and fibrous septa) is now recognized as the most important finding in the diagnosis of the well-differentiated type of early hepatocellular carcinomas (HCCs). In differentiating stromal invasion from pseudoinvasion (benign hepatic tissue in fibrous stroma), the following 5 items are useful: (1) macroscopic or panoramic views of the histological specimen, (2) the amount of fibrous components of stroma, (3) destruction of the structure of portal tracts, (4) loss of reticulin fibers around cancer cells, and (5) cytokeratin 7 immunostaining for ductular proliferation. Knowledge of stromal invasion is also useful for a better understanding of the vasculature (hypovascular HCCs) and histological features (fatty change) of early HCCs. Invasion of preexisting arteries and portal veins causes hypo-vascularity of HCCs. Further, hypovascularity causes fatty change as a hypoxic change of cancer tissues.
Figures



Similar articles
-
Histological features of early hepatocellular carcinomas and their developmental process: for daily practical clinical application : Hepatocellular carcinoma.Hepatol Int. 2009 Mar;3(1):283-93. doi: 10.1007/s12072-008-9107-9. Epub 2008 Nov 14. Hepatol Int. 2009. PMID: 19669379 Free PMC article.
-
Ductular reaction is helpful in defining early stromal invasion, small hepatocellular carcinomas, and dysplastic nodules.Cancer. 2007 Mar 1;109(5):915-23. doi: 10.1002/cncr.22460. Cancer. 2007. PMID: 17279586
-
Small hepatocellular carcinoma on magnetic resonance imaging. Relation of signal intensity to angiographic and clinicopathologic findings.Invest Radiol. 1997 Mar;32(3):161-8. doi: 10.1097/00004424-199703000-00005. Invest Radiol. 1997. PMID: 9055129
-
Early hepatocellular carcinoma and dysplastic nodules.Semin Liver Dis. 2005;25(2):133-42. doi: 10.1055/s-2005-871193. Semin Liver Dis. 2005. PMID: 15918142 Review.
-
Clinico-Radio-Pathological and Molecular Features of Hepatocellular Carcinomas with Keratin 19 Expression.Liver Cancer. 2020 Dec;9(6):663-681. doi: 10.1159/000510522. Epub 2020 Oct 23. Liver Cancer. 2020. PMID: 33442539 Free PMC article. Review.
Cited by
-
Advances in Understanding Hepatocellular Carcinoma Vasculature: Implications for Diagnosis, Prognostication, and Treatment.Korean J Radiol. 2024 Oct;25(10):887-901. doi: 10.3348/kjr.2024.0307. Korean J Radiol. 2024. PMID: 39344546 Free PMC article. Review.
-
Evolution of placental invasion and cancer metastasis are causally linked.Nat Ecol Evol. 2019 Dec;3(12):1743-1753. doi: 10.1038/s41559-019-1046-4. Epub 2019 Nov 25. Nat Ecol Evol. 2019. PMID: 31768023 Free PMC article.
-
Current Concepts of Precancerous Lesions of Hepatocellular Carcinoma: Recent Progress in Diagnosis.Diagnostics (Basel). 2023 Mar 23;13(7):1211. doi: 10.3390/diagnostics13071211. Diagnostics (Basel). 2023. PMID: 37046429 Free PMC article. Review.
-
Characterizing the Invasive Tumor Front of Aggressive Uterine Adenocarcinoma and Leiomyosarcoma.Front Cell Dev Biol. 2021 Jun 3;9:670185. doi: 10.3389/fcell.2021.670185. eCollection 2021. Front Cell Dev Biol. 2021. PMID: 34150764 Free PMC article.
References
-
- International Consensus Group for Hepatocellular Neoplasia. Pathologic diagnosis of early hepatocellular carcinoma: a report of the international consensus group for hepatocellular neoplasia. Hepatology. 2009;49(2):658–664. - PubMed
-
- Kondo Y, Kondo F, Wada K, Okabayashi A. Pathological features of small hepatocellular carcinoma. Acta Pathologica Japonica. 1986;36(8):1149–1161. - PubMed
-
- Kondo F, Kondo Y, Nagato Y, Tomizawa M, Wada K. Interstitial tumour cell invasion in small hepatocellular carcinoma. Evaluation in microscopic and low magnification views. Journal of Gastroenterology and Hepatology. 1994;9(6):604–612. - PubMed
-
- Tomizawa M, Kondo F, Kondo Y. Growth patterns and interstitial invasion of small hepatocellular carcinoma. Pathology International. 1995;45(5):352–358. - PubMed
-
- Nakano M, Saito A, Yamamoto M, Doi M, Takasaki K. Stromal and blood vessel wall invasion in well-differentiated hepatocellular carcinoma. Liver. 1997;17(1):41–46. - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
