

Changes in dipolar structure of cardiac magnetic field maps after ST elevation myocardial infarction
- PMID: 22008494
- PMCID: PMC6932076
- DOI: 10.1111/j.1542-474X.2011.00466.x
Changes in dipolar structure of cardiac magnetic field maps after ST elevation myocardial infarction
Abstract
Background: Pathological changes in cardiac electrophysiology have been investigated in coronary artery disease using magnetocardiography. Aim of this work was to examine the structure of cardiac magnetic field maps (MFM) during ventricular depolarization and repolarization in patients with acute ST elevation myocardial infarction (STEMI).
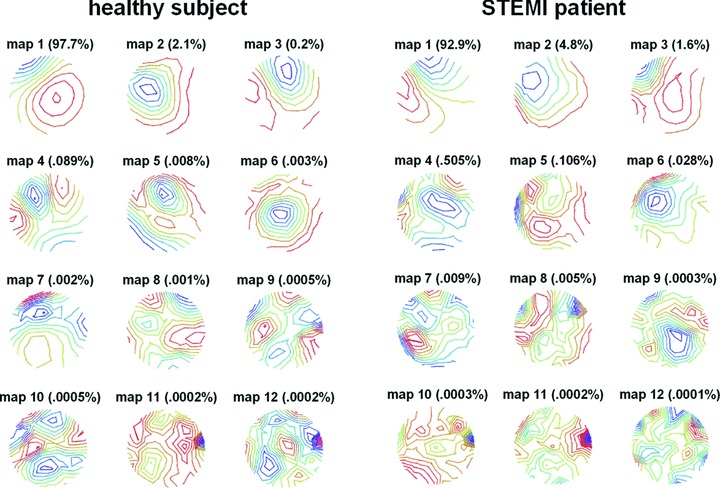
Methods: Magnetocardiograms were recorded in 39 healthy subjects and 97 patients who had been successfully revascularized after STEMI. Using the Karhunen-Loeve transform, 12 eigenmaps were constructed for six intervals within the QT interval of each subject's signal-averaged data. The relative information content of the eigenmaps was compared between STEMI patients and healthy subjects.
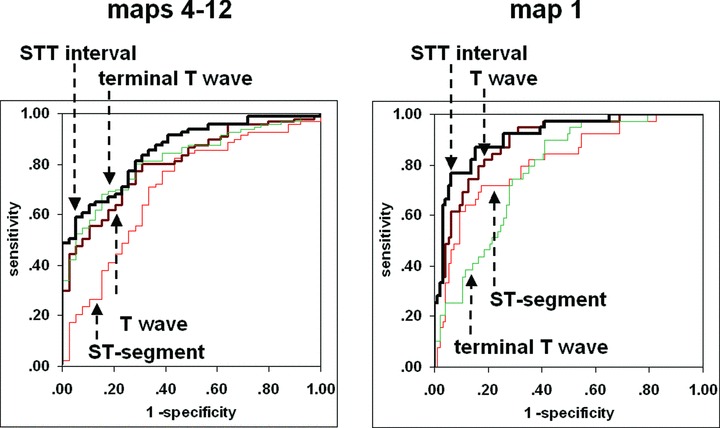
Results: Relative nondipolar content was between 0.03% and 0.52% higher in the STEMI group, (P < 0.001 for the repolarization intervals). Information content of the first dipolar eigenmap in the STEMI group was reduced by 2.6%-11.7% (P < 0.001 for the repolarization intervals). STT interval was best able to discriminate between groups: area-under-the-curve for nondipolar content was 85.8% (P < 0.001), for the first eigenmap 91.7% (P < 0.001). Severity of infarction was reflected in lower STT interval map 1 content for patients with anterior versus posterior infarction (83%± 11% vs. 87%± 10%, P < 0.05), with wall motion disturbances (84%± 11% vs. 92%± 7%, P < 0.001) and with microvascular obstruction (81%± 12% vs. 87%± 10%, P < 0.05). Regression analysis showed that patients with lower ejection fraction tended to have less information content (P < 0.001).
Conclusion: STEMI is associated with a loss of spatial coherence during repolarization, as quantified by principal component analysis of cardiac MFM.
©2011, Wiley Periodicals, Inc.
Figures
References
-
- Koch H. SQUID magnetocardiography: Status and perspectives. IEEE Trans Appl Superconduct 2001;11:49–59.
-
- Lant J, Stroink G, ten Voorde B, et al Complementary nature of electrocardiographic and magnetocardiographic data inpatients with ischemic heart disease. J Electrocardiol 1990;23:315–322. - PubMed
-
- Stroink G, Hailer B, Van Leeuwen P. Cardiomagnetism In Andrä W, Nowak H. (eds.): Magnetism in Medicine. Weinheim , Wiley‐VCH, 2006, pp. 164–209.
-
- Hänninen H, Takala P, Mäkijärvi M, et al Recording locations in multichannel magnetocardiography and body surface potential mapping sensitive for regional exercise‐induced myocardial ischemia. Basic Res Cardiol 2001;96:405–414. - PubMed
-
- Hailer B, Van Leeuwen P, Lange S, et al Spatial dispersion of the magnetocardiographically determined QT intervals and its components in the identification of patients at risk for arrhythmia after myocardial infarction. Ann Noninvasive Electrocardiol 1998;3:311–318.
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
