

Newer drugs and earlier treatment: impact on lifetime cost of care for HIV-infected adults
- PMID: 22008655
- PMCID: PMC3237010
- DOI: 10.1097/QAD.0b013e32834dce6e
Newer drugs and earlier treatment: impact on lifetime cost of care for HIV-infected adults
Abstract
Objective: To determine the component costs of care to optimize treatment with limited resources.
Design: We used the Cost-Effectiveness of Preventing AIDS Complications Model of HIV disease and treatment to project life expectancy and both undiscounted and discounted lifetime costs (2010 €).
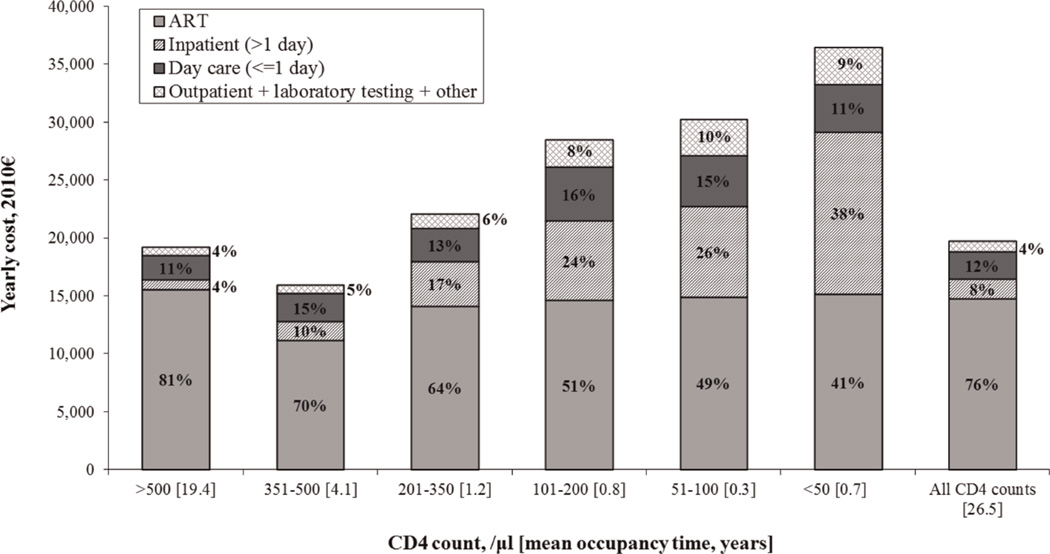
Methods: We determined medical resource utilization among HIV-infected adults followed from 1998 to 2005 in northern France. Monthly HIV costs were stratified by CD4 cell count. Costs of CD4, HIV RNA and genotype tests and antiretroviral therapy (ART) were derived from published literature. Model inputs from national data included mean age 38 years, mean initial CD4 cell count 372 cells/μl, ART initiation at CD4 cell counts less than 350 cells/μl, and ART regimen costs ranging from €760 to 2570 per month.
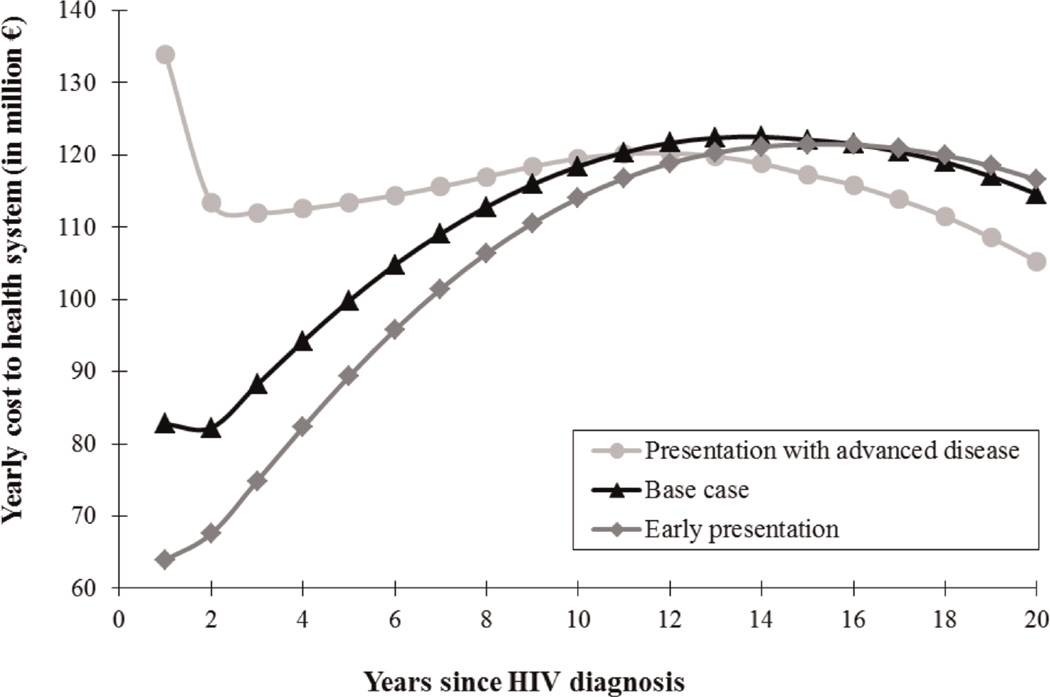
Results: The model projected a mean undiscounted life expectancy of 26.5 years and a lifetime undiscounted cost of €535,000/patient (€320,700 discounted); 73% of costs were ART related. When patients presented to care with mean CD4 cell counts of 510 cells/μl and initiated ART at CD4 cell counts less than 500 cells/μl or HIV RNA more than 100,000 copies/ml, life expectancy was 27.4 years and costs increased 1-2%, to €546,700 (€324,500 discounted). When we assumed introducing generic drugs would result in a 50% decline in first-line ART costs, lifetime costs decreased 4-6%, to €514,200 (€302 ,800 discounted).
Conclusion: As HIV disease is treated earlier with more efficacious drugs, survival and thus costs of care will continue to increase. The availability in high-income countries of widely used antiretroviral drugs in generic form could reduce these costs.
Conflict of interest statement
With the exception of Yazdan Yazdanpanah, none of the authors report any association that might pose a conflict of interest (e.g. pharmaceutical stock ownership, consultancy, advisory board membership, relevant patents, or research funding). Dr. Yazdanpanah has received travel grants, honoraria for presentation at workshops and consultancy honoraria from Bristol-Myers Squibb, Gilead, Merck, Pfizer, Roche and Tibotec, ViiV Healthcare.
Figures
References
-
- Jaggy C, von Overbeck J, Ledergerber B, Schwarz C, Egger M, Rickenbach M, et al. Mortality in the Swiss HIV Cohort Study (SHCS) and the Swiss general population. Lancet. 2003;362:877–878. - PubMed
-
- Lohse N, Hansen AB, Pedersen G, Kronborg G, Gerstoft J, Sorensen HT, et al. Survival of persons with and without HIV infection in Denmark, 1995–2005. Ann Intern Med. 2007;146:87–95. - PubMed
-
- Bhaskaran K, Hamouda O, Sannes M, Boufassa F, Johnson AM, Lambert PC, et al. Changes in the risk of death after HIV seroconversion compared with mortality in the general population. JAMA. 2008;300:51–59. - PubMed
-
- Prise en charge médicale des personnes infectées par le VIH: Rapport 2008. [Accessed September 30, 2008];Flammarion. 2008 at http://www.ladocumentationfrancaise.fr/rapports-publics/084000593/
-
- Thompson MA, Aberg JA, Cahn P, Montaner JS, Rizzardini G, Telenti A, et al. Antiretroviral treatment of adult HIV infection: 2010 recommendations of the International AIDS Society-USA panel. JAMA. 304:321–333. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
