

Risk prediction models for hospital readmission: a systematic review
- PMID: 22009101
- PMCID: PMC3603349
- DOI: 10.1001/jama.2011.1515
Risk prediction models for hospital readmission: a systematic review
Abstract
Context: Predicting hospital readmission risk is of great interest to identify which patients would benefit most from care transition interventions, as well as to risk-adjust readmission rates for the purposes of hospital comparison.
Objective: To summarize validated readmission risk prediction models, describe their performance, and assess suitability for clinical or administrative use.
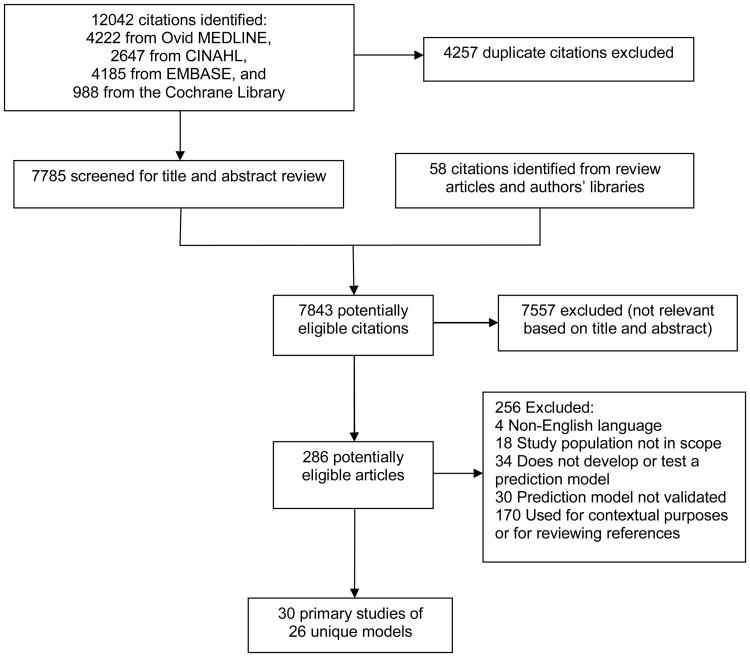
Data sources and study selection: The databases of MEDLINE, CINAHL, and the Cochrane Library were searched from inception through March 2011, the EMBASE database was searched through August 2011, and hand searches were performed of the retrieved reference lists. Dual review was conducted to identify studies published in the English language of prediction models tested with medical patients in both derivation and validation cohorts.
Data extraction: Data were extracted on the population, setting, sample size, follow-up interval, readmission rate, model discrimination and calibration, type of data used, and timing of data collection.
Data synthesis: Of 7843 citations reviewed, 30 studies of 26 unique models met the inclusion criteria. The most common outcome used was 30-day readmission; only 1 model specifically addressed preventable readmissions. Fourteen models that relied on retrospective administrative data could be potentially used to risk-adjust readmission rates for hospital comparison; of these, 9 were tested in large US populations and had poor discriminative ability (c statistic range: 0.55-0.65). Seven models could potentially be used to identify high-risk patients for intervention early during a hospitalization (c statistic range: 0.56-0.72), and 5 could be used at hospital discharge (c statistic range: 0.68-0.83). Six studies compared different models in the same population and 2 of these found that functional and social variables improved model discrimination. Although most models incorporated variables for medical comorbidity and use of prior medical services, few examined variables associated with overall health and function, illness severity, or social determinants of health.
Conclusions: Most current readmission risk prediction models that were designed for either comparative or clinical purposes perform poorly. Although in certain settings such models may prove useful, efforts to improve their performance are needed as use becomes more widespread.
Figures
References
-
- Coleman EA, Parry C, Chalmers S, et al. The care transitions intervention: results of a randomized controlled trial. Arch Intern Med. 2006 Sep 25;166(17):1822–1828. - PubMed
-
- Naylor MD, Brooten D, Campbell R, et al. Comprehensive discharge planning and home follow-up of hospitalized elders: a randomized clinical trial. Jama. 1999 Feb 17;281(7):613–620. - PubMed
-
- QualityNet. [Accessed 5/28/2011];Readmission Measures Overview - Publicly reporting risk-standardized, 30-day readmission measures for AMI, HF and PN. http://www.qualitynet.org/dcs/ContentServer?cid=1219069855273&pagename=Q....
-
- Krumholz HM, Brindis RG, Brush JE, et al. Standards for statistical models used for public reporting of health outcomes: an American Heart Association Scientific Statement from the Quality of Care and Outcomes Research Interdisciplinary Writing Group: cosponsored by the Council on Epidemiology and Prevention and the Stroke Council. Endorsed by the American College of Cardiology Foundation. Circulation. 2006 Jan 24;113(3):456–462. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
