

Cellular and molecular mechanisms of renal fibrosis
- PMID: 22009250
- PMCID: PMC4520424
- DOI: 10.1038/nrneph.2011.149
Cellular and molecular mechanisms of renal fibrosis
Abstract
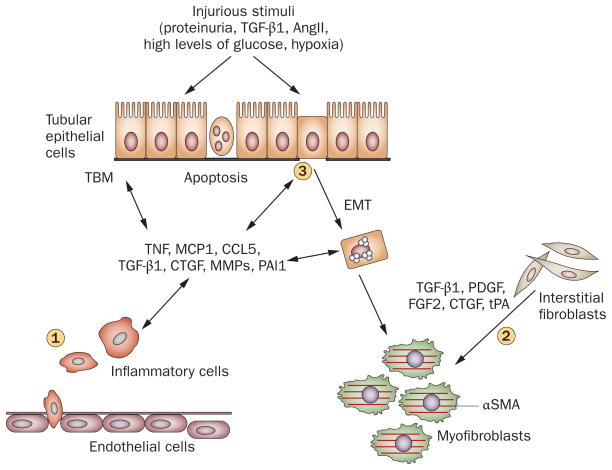
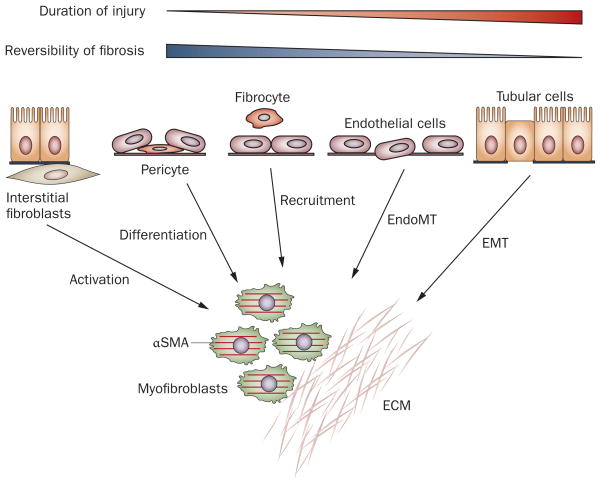
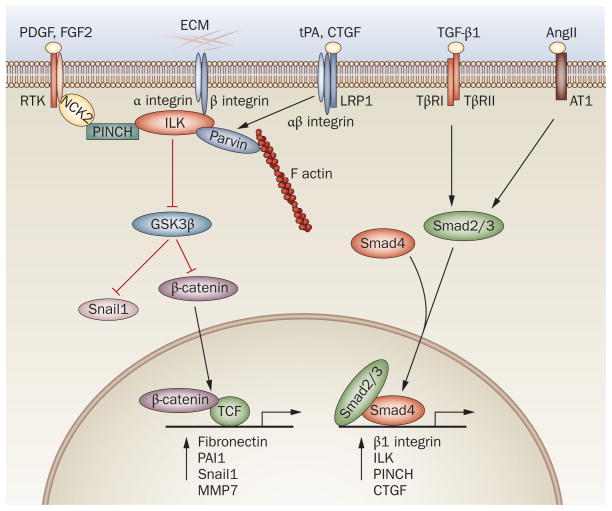
Renal fibrosis, particularly tubulointerstitial fibrosis, is the common final outcome of almost all progressive chronic kidney diseases. Renal fibrosis is also a reliable predictor of prognosis and a major determinant of renal insufficiency. Irrespective of the initial causes, renal fibrogenesis is a dynamic and converging process that consists of four overlapping phases: priming, activation, execution and progression. Nonresolving inflammation after a sustained injury sets up the fibrogenic stage (priming) and triggers the activation and expansion of matrix-producing cells from multiple sources through diverse mechanisms, including activation of interstitial fibroblasts and pericytes, phenotypic conversion of tubular epithelial and endothelial cells and recruitment of circulating fibrocytes. Upon activation, matrix-producing cells assemble a multicomponent, integrin-associated protein complex that integrates input from various fibrogenic signals and orchestrates the production of matrix components and their extracellular assembly. Multiple cellular and molecular events, such as tubular atrophy, microvascular rarefaction and tissue hypoxia, promote scar formation and ensure a vicious progression to end-stage kidney failure. This Review outlines our current understanding of the cellular and molecular mechanisms of renal fibrosis, which could offer novel insights into the development of new therapeutic strategies.
Conflict of interest statement
The author declares no competing interests.
Figures
References
-
- Coresh J, et al. Prevalence of chronic kidney disease in the United States. JAMA. 2007;298:2038–2047. - PubMed
-
- United States Renal Data System. Annual Data Report 2009. 2010 [online], http://www.usrds.org/adr.htm.
-
- Sharma SK, et al. Burden of CKD, proteinuria, and cardiovascular risk among Chinese, Mongolian, and Nepalese participants in the International Society of Nephrology screening programs. Am J Kidney Dis. 2010;56:915–927. - PubMed
-
- Zhang L, et al. Prevalence and factors associated with CKD: a population study from Beijing. Am J Kidney Dis. 2008;51:373–384. - PubMed
-
- Liu Y. Renal fibrosis: new insights into the pathogenesis and therapeutics. Kidney Int. 2006;69:213–217. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
