

Review of current treatment of sacral chordoma
- PMID: 22009849
- PMCID: PMC6583561
- DOI: 10.1111/j.1757-7861.2009.00027.x
Review of current treatment of sacral chordoma
Abstract
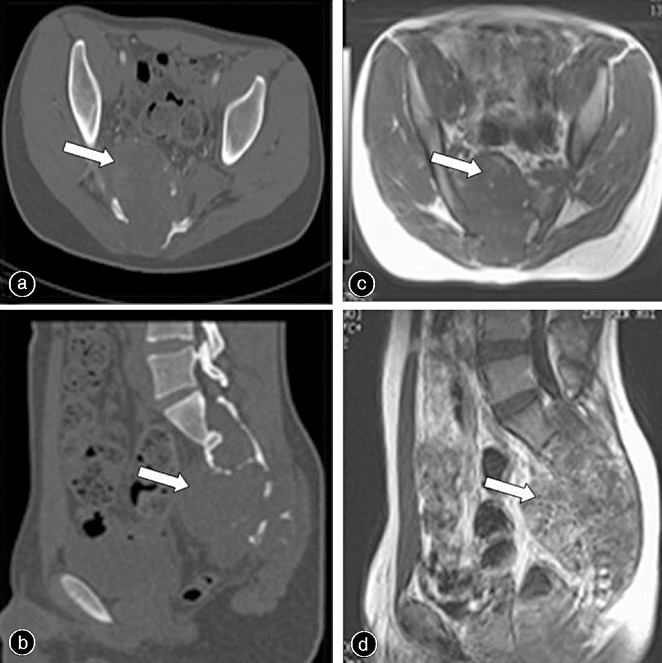
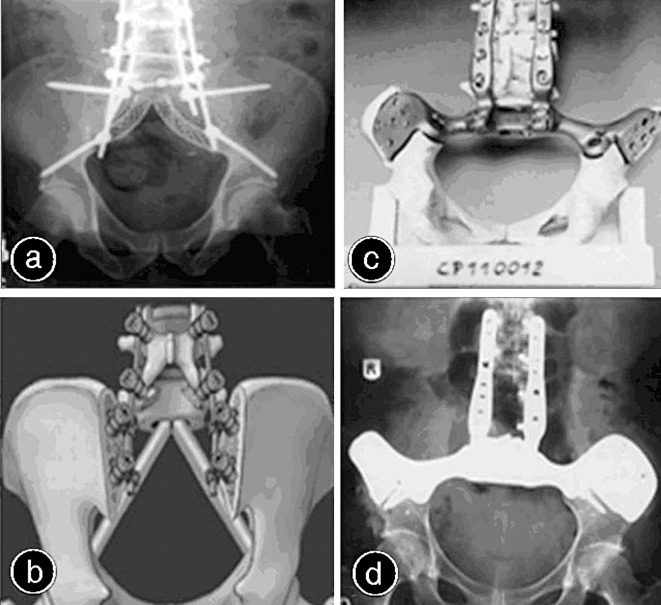
Chordoma is a relatively rare, locally aggressive tumor which is known to arise from embryonic remnants of the notochord and to occur exclusively along the spinal axis, with a predilection for the sacrum. Although chordoma typically presents as a single lesion, a few cases of metastasis have been reported and the prognosis of such patients may be poor. Chordomas are slowly growing tumors with insidious onset of symptoms, making early diagnosis difficult. Recent improvements in imaging have provided valuable information for early diagnosis. The optimal treatment for sacral chordoma is en bloc sacral resection with wide surgical margins. Improvement in surgical techniques has widened the opportunities to provide effective treatment. However, the effects of adjuvant treatment options are still both unclear and controversial. Substantial progress has been made in the study of molecular-targeted therapy. The authors review the current surgical and adjuvant treatment modalities, including molecular-targeted therapy, available for management of sacral chordoma.
© 2009 Tianjin Hospital and Blackwell Publishing Asia Pty Ltd.
Figures
Similar articles
-
Current management of sacral chordoma.Neurosurg Focus. 2003 Aug 15;15(2):E9. doi: 10.3171/foc.2003.15.2.9. Neurosurg Focus. 2003. PMID: 15350040 Review.
-
Multidisciplinary approach of lumbo-sacral chordoma: From oncological treatment to reconstructive surgery.J Surg Oncol. 2015 Oct;112(5):544-54. doi: 10.1002/jso.24026. J Surg Oncol. 2015. PMID: 26496212 Review.
-
Surgical Treatment of Sacral Chordoma: En Bloc Resection with Negative Margins is a Determinant of the Long-Term Outcome.Surg Technol Int. 2018 Nov 11;33:343-348. Surg Technol Int. 2018. PMID: 30204925
-
A review of the surgical management of sacral chordoma.Eur J Surg Oncol. 2014 Nov;40(11):1412-20. doi: 10.1016/j.ejso.2014.04.008. Epub 2014 Apr 25. Eur J Surg Oncol. 2014. PMID: 24793103 Review.
-
[Clinico-diagnostic aspects and therapeutic considerations of the combined surgical and radiotherapeutic approach in 2 cases of sacrococcygeal chordoma: our experience].G Chir. 1997 Mar;18(3):107-10. G Chir. 1997. PMID: 9206489 Italian.
Cited by
-
Sacral chordoma: challenging for resection margin.Ann Coloproctol. 2014 Jun;30(3):104-5. doi: 10.3393/ac.2014.30.3.104. Ann Coloproctol. 2014. PMID: 24999457 Free PMC article. No abstract available.
-
Low expression of PHLPP1 in sacral chordoma and its association with poor prognosis.Int J Clin Exp Pathol. 2015 Nov 1;8(11):14741-8. eCollection 2015. Int J Clin Exp Pathol. 2015. PMID: 26823799 Free PMC article.
-
Active receptor tyrosine kinases, but not Brachyury, are sufficient to trigger chordoma in zebrafish.Dis Model Mech. 2019 Jul 16;12(7):dmm039545. doi: 10.1242/dmm.039545. Dis Model Mech. 2019. PMID: 31221659 Free PMC article.
-
Case report: Successful treatment of recurrent chordoma and bilateral pulmonary metastases following an 11-year disease-free period.Int J Surg Case Rep. 2014;5(7):424-7. doi: 10.1016/j.ijscr.2014.02.005. Epub 2014 May 2. Int J Surg Case Rep. 2014. PMID: 24907541 Free PMC article.
-
Risk Factors Associated with Reconstructive Complications Following Sacrectomy.Plast Reconstr Surg Glob Open. 2018 Nov 5;6(11):e2002. doi: 10.1097/GOX.0000000000002002. eCollection 2018 Nov. Plast Reconstr Surg Glob Open. 2018. PMID: 30881800 Free PMC article.
References
-
- Samson IR, Springfield DS, Suit HD, et al. Operative treatment of sacrococcygeal chordoma. A review of twenty‐one cases. J Bone Joint Surg Am, 1993, 75: 1476–1484. - PubMed
-
- Chandawarkar RY. Sacrococcygeal chordoma: review of 50 consecutive patients. World J Surg, 1996, 20: 717–719. - PubMed
-
- Enneking WF. A system of staging musculoskeletal neoplasms. Clin Orthop Relat Res, 1986, 204: 9–24. - PubMed
-
- Yamaguchi T, Yamato M, Saotome K. First histologically confirmed case of a classic chordoma arising in a precursor benign notochordal lesion: differential diagnosis of benign and malignant notochordal lesions. Skeletal Radiol, 2002, 31: 413–418. - PubMed
-
- Bergh P, Kindblom LG, Gunterberg B, et al. Prognostic factors in chordoma of the sacrum and mobile spine: a study of 39 patients. Cancer, 2000, 88: 2122–2134. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
