

Diagnosis and treatment of excessive lateral pressure syndrome of the patellofemoral joint caused by military training
- PMID: 22009978
- PMCID: PMC6583146
- DOI: 10.1111/j.1757-7861.2010.00116.x
Diagnosis and treatment of excessive lateral pressure syndrome of the patellofemoral joint caused by military training
Abstract
Objective: To investigate the diagnosis and surgical treatment of excessive lateral pressure syndrome of the patellofemoral joint caused by military training.
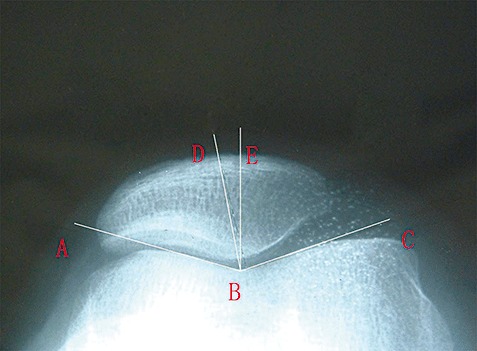
Methods: Fifteen patients (patient group) and 18 healthy volunteers (control group) were involved in this retrospective study. Radiographs of the knee joints of all patients and volunteers were taken. The bone architecture was assessed, the trochlear angle, coincidence angle and patellofemoral joint index measured in both groups, and the resulting data compared. All 15 patients (17 knees) were treated by lateral collateral retinaculum release. Pre- and post-operative pain was evaluated with a visual analog scale (VAS).
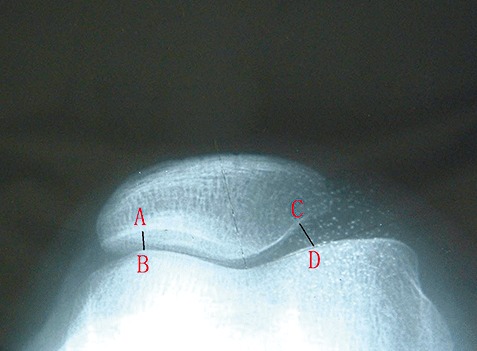
Results: The differences between the two groups in coincidence angle (patient group: 7.67°± 5.81°; control group: -2.2°±-2.71°) and patellofemoral joint index (patient group: 2.49 ± 1.40; control group: 1.25 ± 0.15) were statistically significant. Subchondral bone sclerosis and osteophytosis in the patellofemoral joint were more pronounced in the patient group than in the control group. The VAS was higher preoperatively (7.06 ± 0.85) than postoperatively (6 months postoperatively: 3.87 ± 0.24; 1 year postoperatively: 3.01 ± 0.17), and the differences between preoperative and postoperative were statistically significant.
Conclusions: Apart from the case history, typical symptoms and physical signs, X-ray examination is the most basic way to diagnose excessive lateral pressure syndrome of the patellofemoral joint, and the patellofemoral joint index is the most reliable for diagnosis. Lateral collateral retinaculum release with a small-incision is an effective treatment for this disease.
© 2011 Tianjin Hospital and Blackwell Publishing Asia Pty Ltd.
Figures

References
-
- Lv HS. Surgery of the Knee, 3rd edn. Beijing: People Medicine Publishing House, 2006; 894, 897, 911–912.
-
- Merchant AC, Mercer RL, Jacobsen RH, et al Roentgenographic analysis of patellofemoral congruence. J Bone Joint Surg Am, 1974, 56: 1391–1396. - PubMed
-
- Laurin CA, Dussault R, Levesque HP. The tangential X‐ray investigation of the patellofemoral joint: X‐ray technique, diagnostic criteria and their interpretation. Clin Orthop Relat Res, 1979, 144: 16–26. - PubMed
-
- Hughston JC, Flandry F, Brinker MR, et al Surgical correction of medial subluxation of the patella. Am J Sports Med, 1996, 24: 486–491. - PubMed
-
- Merchant AC. Classification of patellofemoral disorders. Arthroscopy, 1988, 4: 235–240. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
