

Transthoracic fine-needle aspiration biopsy of the lungs using a C-arm cone-beam CT system: diagnostic accuracy and post-procedural complications
- PMID: 22010033
- PMCID: PMC3474125
- DOI: 10.1259/bjr/64727750
Transthoracic fine-needle aspiration biopsy of the lungs using a C-arm cone-beam CT system: diagnostic accuracy and post-procedural complications
Abstract
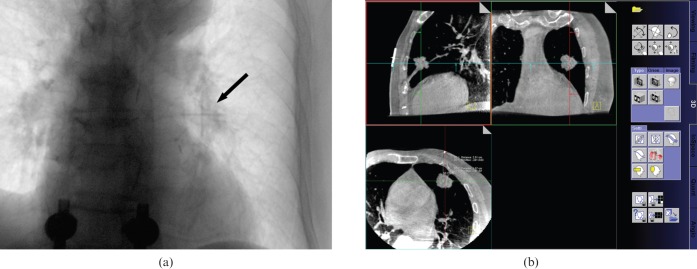
Objective: The purpose of our study was to evaluate the diagnostic accuracy of transthoracic fine-needle aspiration biopsy (TFNAB) using a C-arm cone-beam CT (CBCT) system and to assess risk factors for immediate post-procedural complications in patients with lung lesions.
Methods: From October 2007 to April 2009, 94 TFNAB procedures using a C-arm system were studied in 91 patients with pulmonary lesions a chest CT scans. We retrospectively reviewed the patients' radiological and histopathological findings. We evaluated the lesion size, lesion abutted to pleura and presence or absence of emphysema along the needle path, lesion depth, visibility of target lesion and patient's position. Pneumothorax and pulmonary haemorrhage were assessed after TFNAB. Overall diagnostic accuracy, sensitivity, specificity, positive predictive value (PPV) and negative predictive value (NPV) were analysed.
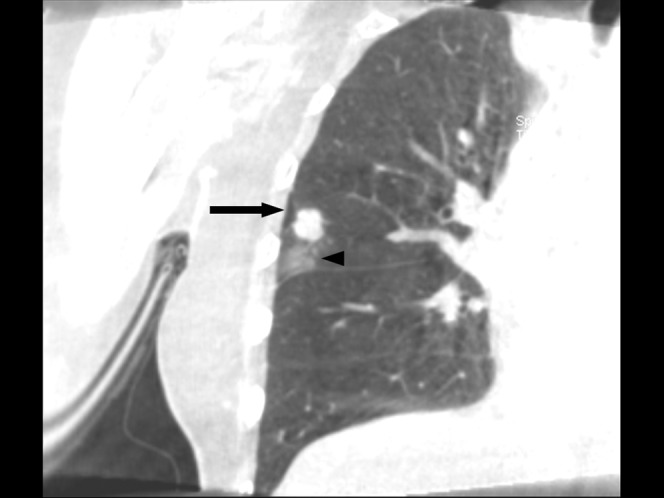
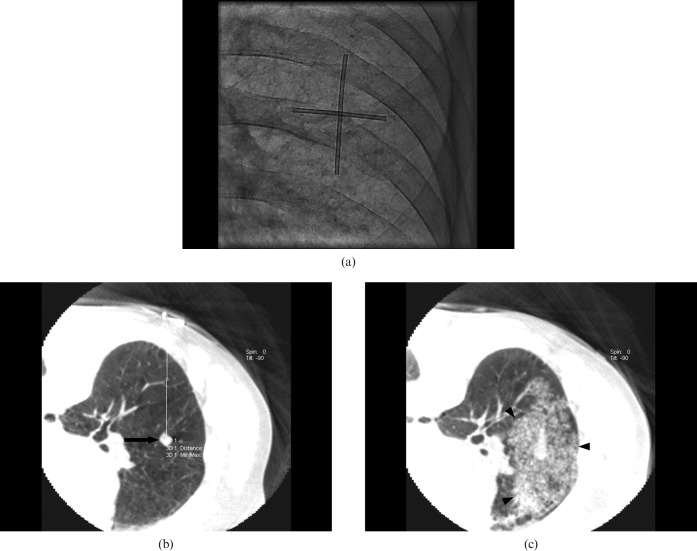
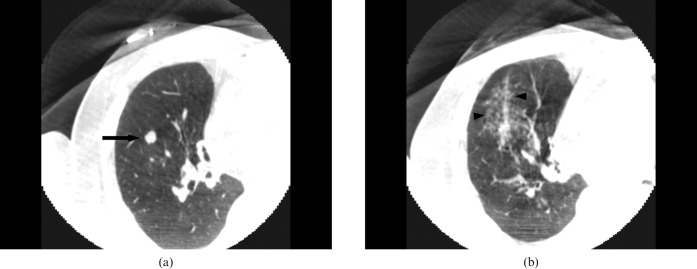
Results: In 94 TFNAB procedures, 58 lesions were malignant and 36 were benign. The sensitivity, specificity, PPV, NPV and overall diagnostic accuracy rate of TFNAB were 93.1%, 100%, 100%, 90% and 97.9%, respectively. Pneumothorax was developed in 24 procedures. None of the parameters showed significant impact on the frequency of the pneumothorax. Overall haemorrhage occurred in 43 procedures. The incidence of overall haemorrhage was higher in patients with smaller lesions, longer pleural distance and pleural abutted lesions (p<0.05). Differences in visibility at projection radiographs were statistically significant between patients with or without perilesional haemorrhage (p<0.05).
Conclusion: Transthoracic fine-needle aspiration biopsy using a C-arm CBCT system is feasible for imaging guidance of lung lesion and early detection of the procedural-related complications.
Figures
References
-
- Kurban LA, Gomersall L, Weir J, Wade P. Fluoroscopy-guided percutaneous lung biopsy: a valuable alternative to computed tomography. Acta Radiol 2008;49:876–82 - PubMed
-
- Li H, Boiselle PM, Shepard JO, Trotman-Dickenson B, McLoud TC. Diagnostic accuracy and safety of CT-guided percutaneous needle aspiration biopsy of the lung: comparison of small and large pulmonary nodules. AJR Am J Roentgenol 1996;167:105–9 - PubMed
-
- Heyer CM, Reichelt S, Peters SA, Walther JW, Muller KM, Nicolas V. Computed tomography-navigated transthoracic core biopsy of pulmonary lesions: which factors affect diagnostic yield and complication rates? Acad Radiol 2008;15:1017–26 - PubMed
-
- Goldberg SN, Keogan MT, Raptopoulos V. Percutaneous CT-guided biopsy: improved confirmation of sampling site and needle positioning using a multistep technique at CT fluoroscopy. J Comput Assist Tomogr 2000;24:264–6 - PubMed
-
- Heck SL, Blom P, Berstad A. Accuracy and complications in computed tomography fluoroscopy-guided needle biopsies of lung masses. Eur Radiol 2006;16:1387–92 - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
