

Intracranial aneurysms: optimized diagnostic tools call for thorough interdisciplinary treatment strategies
- PMID: 22010040
- PMCID: PMC3187677
- DOI: 10.1177/1756285611415309
Intracranial aneurysms: optimized diagnostic tools call for thorough interdisciplinary treatment strategies
Abstract
Objective: Intracranial aneurysms (IAs) require deliberately selected treatment strategies as they are incrementally found prior to rupture and deleterious subarachnoid haemorrhage (SAH). Multiple and recurrent aneurysms necessitate both neurointerventionalists and neurosurgeons to optimize aneurysmal occlusion in an interdisciplinary effort. The present study was conducted to condense essential strategies from a single neurovascular centre with regard to the lessons learned.
Method: Medical charts of 321 consecutive patients treated for IAs at our centre from September 2008 until December 2010 were retrospectively analysed for clinical presentation of the aneurysms, multiplicity and treatment pathways. In addition, a selective Medline search was performed.
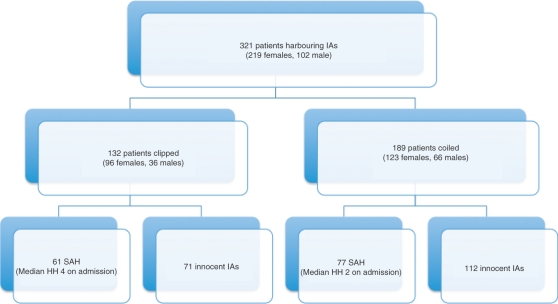
Results: A total of 321 patients with 492 aneurysms underwent occlusion of their symptomatic aneurysm: 132 (41.1%) individuals were treated surgically, 189 (58.2%) interventionally; 138 patients presented with a SAH, of these 44.2% were clipped and 55.8% were coiled. Aneurysms of the middle cerebral artery were primarily occluded surgically (88), whereas most of the aneurysms of the internal carotid artery and anterior communicating artery (114) were treated endovascularly. Multiple aneurysms (range 2-5 aneurysms/individual) were diagnosed in 98 patients (30.2%). During the study period 12 patients with recurrent aneurysms were allocated to another treatment modality (previously clip to coil and vice versa).
Conclusions: Our data show that successful interdisciplinary occlusion of IAs is based on both neurosurgical and neurointerventional therapy. In particular, multiple and recurrent aneurysms require tailored individual approaches to aneurysmal occlusion. This is achieved by a consequent interdisciplinary pondering of the optimal strategy to occlude IAs in order to prevent SAH.
Keywords: clipping; coiling; interdisciplinary treatment; intracranial aneurysms.
Figures





Similar articles
-
Coil embolization for intracranial aneurysms: an evidence-based analysis.Ont Health Technol Assess Ser. 2006;6(1):1-114. Epub 2006 Jan 1. Ont Health Technol Assess Ser. 2006. PMID: 23074479 Free PMC article.
-
Important factors for a combined neurovascular team to consider in selecting a treatment modality for patients with previously clipped residual and recurrent intracranial aneurysms.Neurosurgery. 2003 Apr;52(4):732-8; discussion 738-9. doi: 10.1227/01.neu.0000053209.61909.f2. Neurosurgery. 2003. PMID: 12657168
-
Microsurgical clipping of previously coiled intracranial aneurysms.Clin Neurol Neurosurg. 2013 Aug;115(8):1343-9. doi: 10.1016/j.clineuro.2012.12.030. Epub 2013 Jan 24. Clin Neurol Neurosurg. 2013. PMID: 23352715
-
Treatment of Recurrent Intracranial Aneurysms After Clipping: A Report of 23 Cases and a Review of the Literature.World Neurosurg. 2016 Aug;92:434-444. doi: 10.1016/j.wneu.2016.05.053. Epub 2016 May 27. World Neurosurg. 2016. PMID: 27241096 Review.
-
Pediatric Intracranial Aneurysms: Considerations and Recommendations for Follow-Up Imaging.World Neurosurg. 2018 Jan;109:418-431. doi: 10.1016/j.wneu.2017.09.150. Epub 2017 Oct 3. World Neurosurg. 2018. PMID: 28986225 Review.
Cited by
-
LATE ANEURYSM RELAPSE AFTER MICROSURGICAL TREATMENT OF MIDDLE CEREBRAL ARTERY ANEURYSM: A CASE REPORT AND LITERATURE REVIEW OF TREATMENT OPTIONS.Acta Clin Croat. 2020 Sep;59(3):532-538. doi: 10.20471/acc.2020.59.03.19. Acta Clin Croat. 2020. PMID: 34177065 Free PMC article. Review.
-
Stent-assisted treatment of ruptured intracranial aneurysms in the acute phase: A single center experience.eNeurologicalSci. 2018 Jan 28;10:31-36. doi: 10.1016/j.ensci.2018.01.001. eCollection 2018 Mar. eNeurologicalSci. 2018. PMID: 29736426 Free PMC article.
-
Outcome for unruptured middle cerebral artery aneurysm treatment: surgical and endovascular approach in a single center.Neurosurg Rev. 2014 Oct;37(4):643-51. doi: 10.1007/s10143-014-0563-5. Epub 2014 Jul 9. Neurosurg Rev. 2014. PMID: 25005630
-
Application of zone classification in multiple intracranial aneurysmal subarachnoid hemorrhage treatment strategies.Heliyon. 2024 Feb 22;10(5):e26857. doi: 10.1016/j.heliyon.2024.e26857. eCollection 2024 Mar 15. Heliyon. 2024. PMID: 38434361 Free PMC article.
-
Treatment of complex neurovascular lesions: an interdisciplinary angio suite approach.Ther Adv Neurol Disord. 2014 Jan;7(1):60-70. doi: 10.1177/1756285613496861. Ther Adv Neurol Disord. 2014. PMID: 24409203 Free PMC article.
References
-
- Atlas S.W., Sheppard L., Goldberg H.I., Hurst R.W., Listerud J., Flamm E. (1997) Intracranial aneurysms: detection and characterization with MR angiography with use of an advanced postprocessing technique in a blinded-reader study. Radiology 203: 807–814 - PubMed
-
- Beck J., Raabe A., Szelenyi A., Berkefeld J., Gerlach R., Setzer M., et al. (2006) Sentinel headache and the risk of rebleeding after aneurysmal subarachnoid hemorrhage. Stroke 37: 2733–2737 - PubMed
-
- Bederson J.B., Awad I.A., Wiebers D.O., Piepgras D., Haley E.C., Jr, Brott T., et al. (2000) Recommendations for the management of patients with unruptured intracranial aneurysms: A Statement for healthcare professionals from the Stroke Council of the American Heart Association. Stroke 31: 2742–2750 - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous
