

Depression and rehospitalization following acute myocardial infarction
- PMID: 22010201
- PMCID: PMC3229921
- DOI: 10.1161/CIRCOUTCOMES.111.961896
Depression and rehospitalization following acute myocardial infarction
Abstract
Background: Elevated scores on depression symptom questionnaires predict rehospitalization after acute myocardial infarction (AMI). Whether the Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition, depressive disorders predict rehospitalization after AMI is unknown.
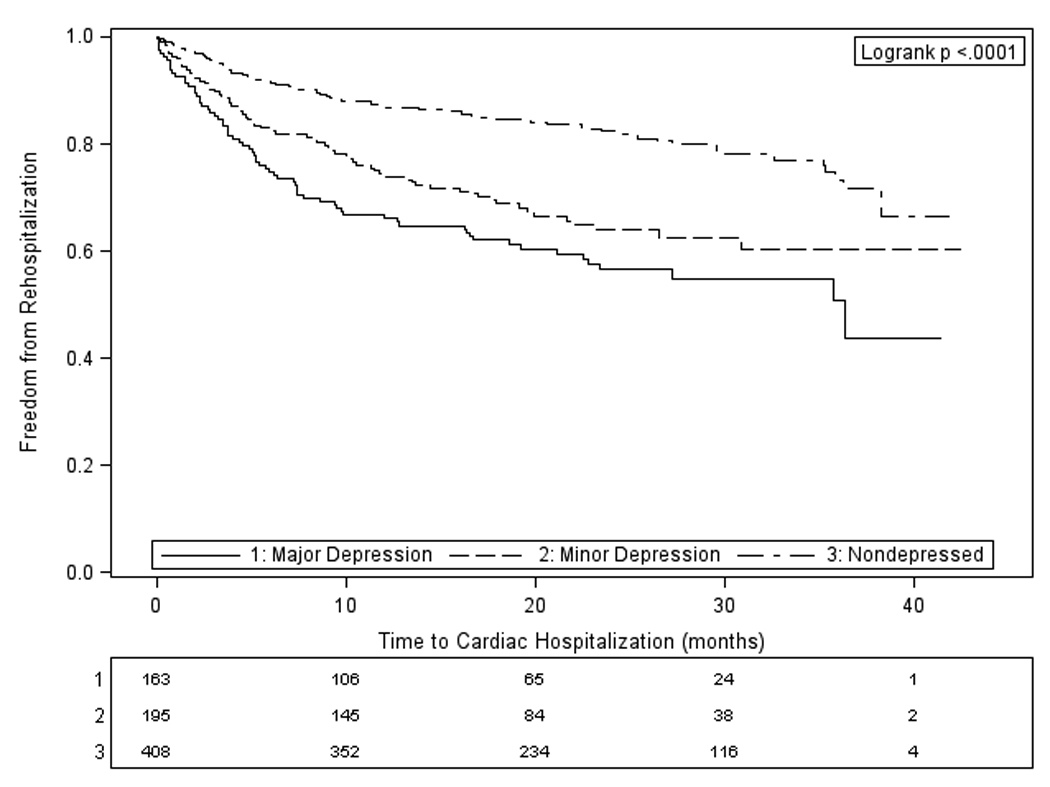
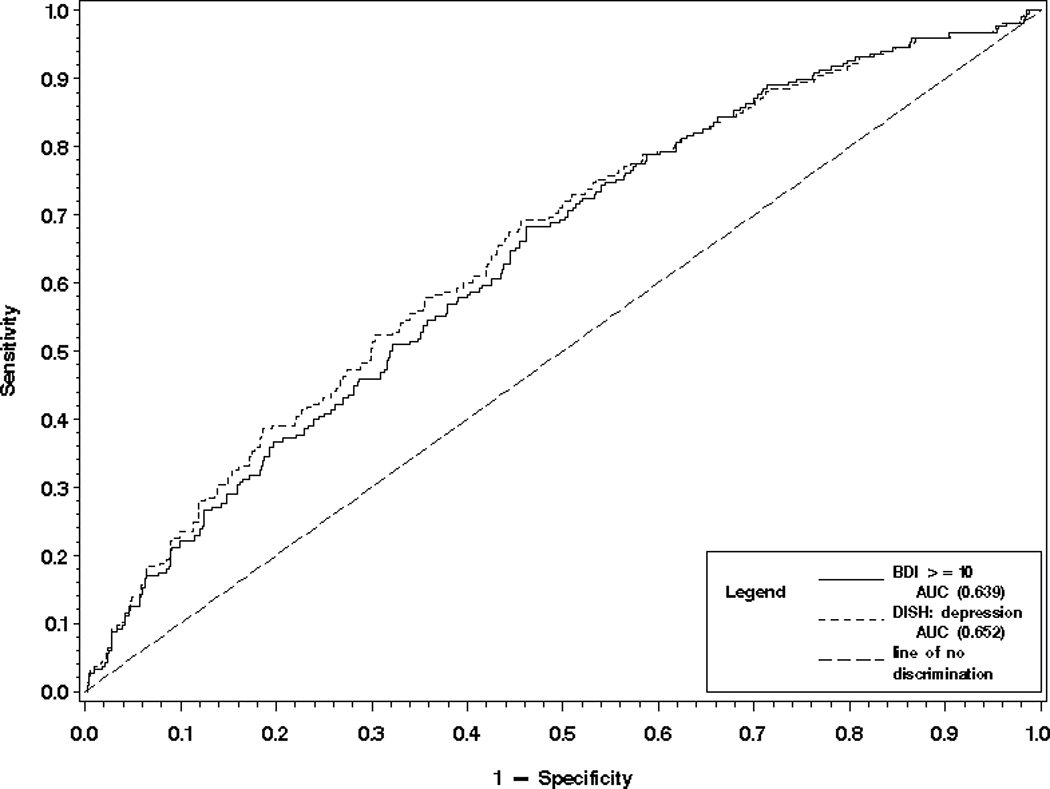
Methods and results: Participants (n=766) in an Enhancing Recovery and Coronary Heart Disease ancillary study were classified by diagnostic interview as having no depression, minor depression, or major depression after AMI. Cardiac rehospitalizations were tracked for up to 42 months. Cox proportional hazards regression was used to model the effect of depressive disorder on time to first cardiac rehospitalization, controlling for mortality risk factors. Logistic regression was used to compare the accuracy with which rehospitalization could be predicted by depression diagnosis or by the Beck Depression Inventory (BDI). Secondary analyses examined the effects of depression on the cumulative number of all-cause rehospitalizations, length of stay, and emergency department visits. Compared with patients without depression, patients with either minor or major depression were hospitalized sooner (minor depression adjusted hazard ratio, 2.22; 95% CI, 1.59-3.08; P<0.001; major depression adjusted hazard ratio, 2.54; 95% CI, 1.84-3.53; P<0.001), had more hospitalizations (minor, P<0.001; major, P<0.001) and emergency department visits (minor, P=0.003; major, P<0.001), and spent more days in the hospital (minor, P<0.001; major, P<0.001). The interview and questionnaire methods of assessing depression did not significantly differ in their overall accuracy of predicting rehospitalization.
Conclusions: Depressive disorders increase the risk of rehospitalization after AMI. Future work should focus on developing multivariable models to predict risk of rehospitalization after AMI, and depression should be included in these.
Conflict of interest statement
Figures
References
-
- Xu J, Kochanek KD, Murphy S, Tejada-Vera B. Deaths: Final Data for 2007. National Vital Statistics Reports. 2010;58 - PubMed
-
- Berenson K, Ogbonnaya A, Casciano R, Makenbaeva D, Mozaffari E, Lamerato L, Corbelli J. Economic consequences of ACS-related rehospitalizations in the US. Current Medical Research and Opinion. 2010;26:329–336. - PubMed
-
- Menzin J, Wygant G, Hauch O, Jackel J, Friedman M. One-year costs of ischemic heart disease among patients with acute coronary syndromes: findings from a multi-employer claims database. Current Medical Research and Opinion. 2008;24:461–468. - PubMed
-
- Johnston SS, Curkendall S, Makenbaeva D, Mozaffari E, Goetzel R, Burton W, Maclean R. The Direct and Indirect Cost Burden of Acute Coronary Syndrome. Journal of Occupational and Environmental Medicine. 2011;53:2–7. - PubMed
-
- Kauf TL, Velazquez EJ, Crosslin DR, Weaver WD, Diaz R, Granger CB, McMurray JJV, Rouleau JL, Aylward PE, White HD, Califf RM, Schulman KA. The cost of acute myocardial infarction in the new millennium: Evidence from a multinational registry. American Heart Journal. 2006;151:206–212. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
