

Timing of antiretroviral therapy for HIV-1 infection and tuberculosis
- PMID: 22010914
- PMCID: PMC3327101
- DOI: 10.1056/NEJMoa1013607
Timing of antiretroviral therapy for HIV-1 infection and tuberculosis
Abstract
Background: Antiretroviral therapy (ART) is indicated during tuberculosis treatment in patients infected with human immunodeficiency virus type 1 (HIV-1), but the timing for the initiation of ART when tuberculosis is diagnosed in patients with various levels of immune compromise is not known.
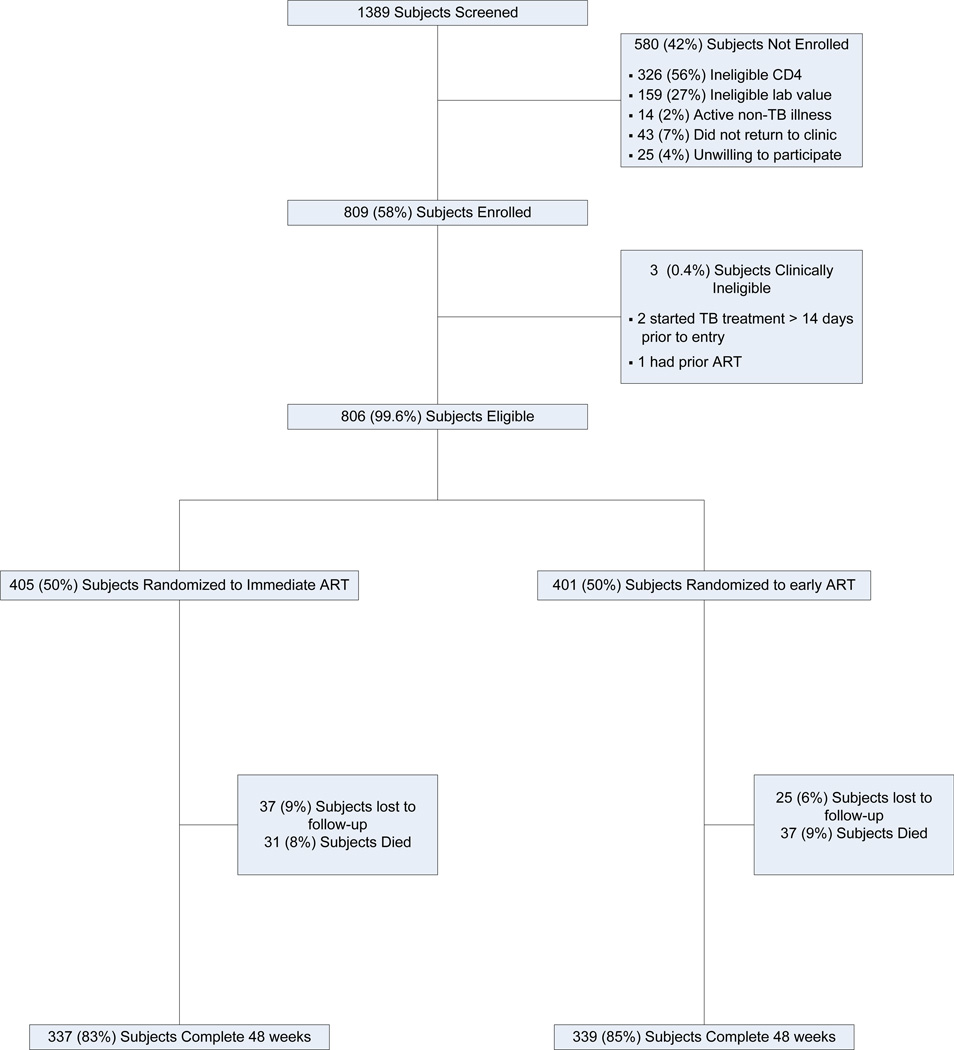
Methods: We conducted an open-label, randomized study comparing earlier ART (within 2 weeks after the initiation of treatment for tuberculosis) with later ART (between 8 and 12 weeks after the initiation of treatment for tuberculosis) in HIV-1 infected patients with CD4+ T-cell counts of less than 250 per cubic millimeter and suspected tuberculosis. The primary end point was the proportion of patients who survived and did not have a new (previously undiagnosed) acquired immunodeficiency syndrome (AIDS)-defining illness at 48 weeks.
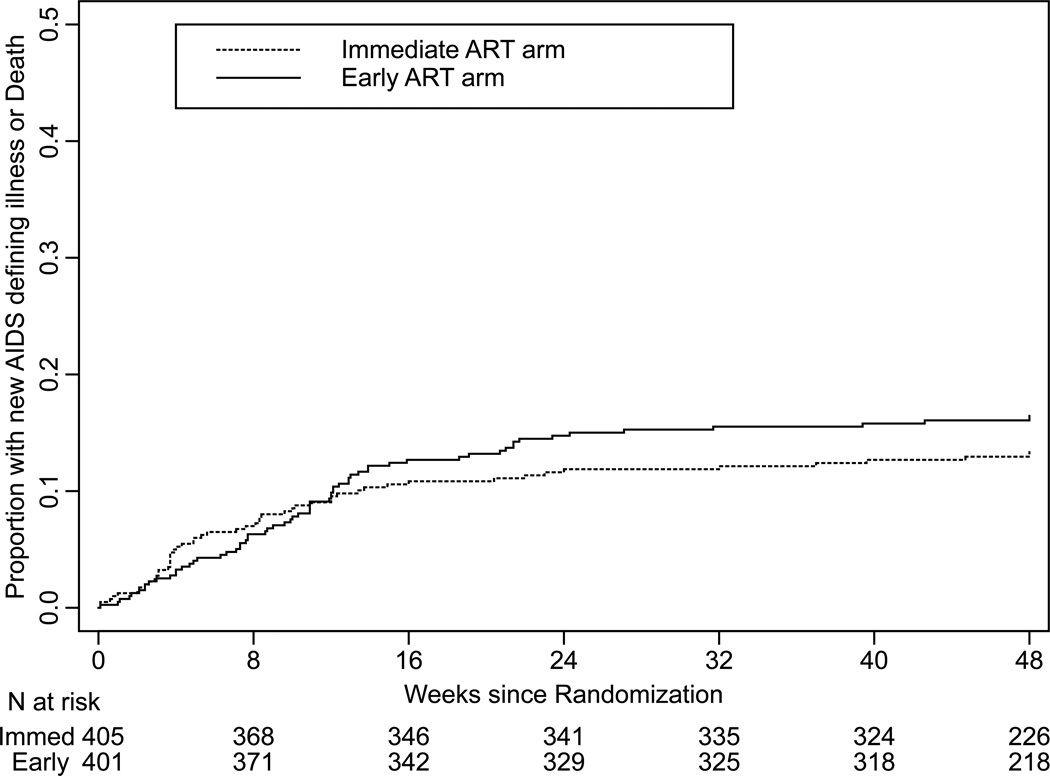
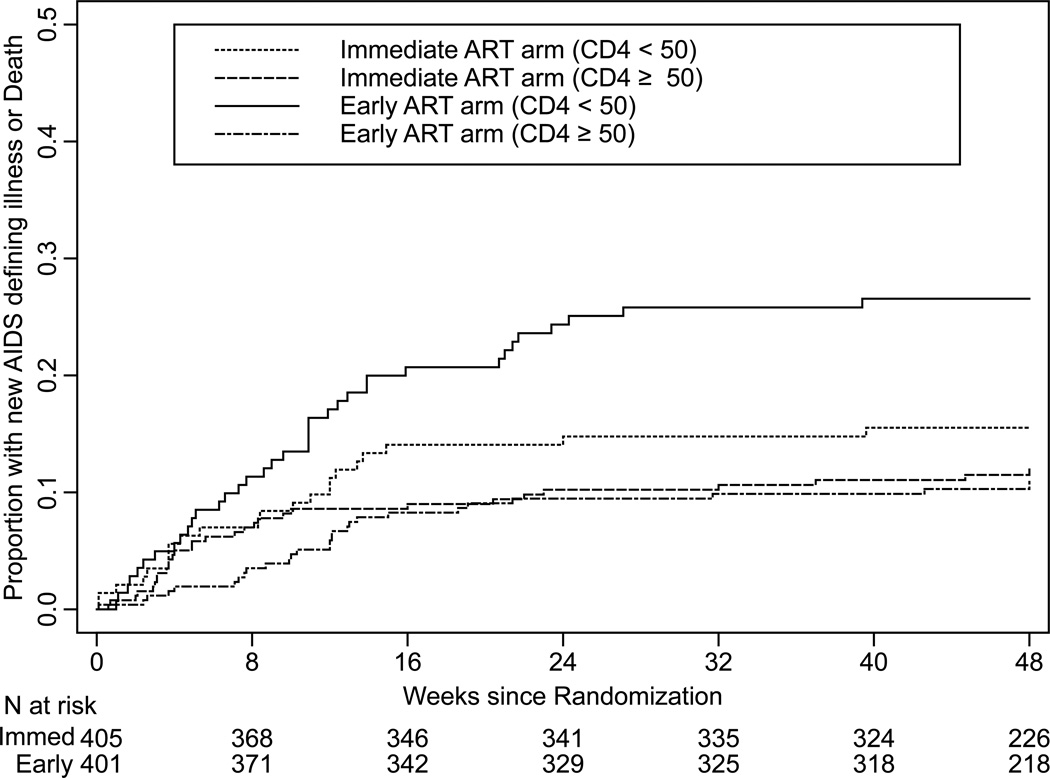
Results: A total of 809 patients with a median baseline CD4+ T-cell count of 77 per cubic millimeter and an HIV-1 RNA level of 5.43 log(10) copies per milliliter were enrolled. In the earlier-ART group, 12.9% of patients had a new AIDS-defining illness or died by 48 weeks, as compared with 16.1% in the later-ART group (95% confidence interval [CI], -1.8 to 8.1; P=0.45). Among patients with screening CD4+ T-cell counts of less than 50 per cubic millimeter, 15.5% of patients in the earlier-ART group versus 26.6% in the later-ART group had a new AIDS-defining illness or died (95% CI, 1.5 to 20.5; P=0.02). Tuberculosis-associated immune reconstitution inflammatory syndrome was more common with earlier ART than with later ART (11% vs. 5%, P=0.002). The rate of viral suppression at 48 weeks was 74% and did not differ between the groups (P=0.38).
Conclusions: Overall, earlier ART did not reduce the rate of new AIDS-defining illness and death, as compared with later ART. In persons with CD4+ T-cell counts of less than 50 per cubic millimeter, earlier ART was associated with a lower rate of new AIDS-defining illnesses and death. (Funded by the National Institutes of Health and others; ACTG A5221 ClinicalTrials.gov number, NCT00108862.).
Figures
Comment in
-
When to start antiretroviral therapy in HIV-associated tuberculosis.N Engl J Med. 2011 Oct 20;365(16):1538-40. doi: 10.1056/NEJMe1109546. N Engl J Med. 2011. PMID: 22010921 No abstract available.
-
Timing of antiretroviral therapy for HIV-1-associated tuberculosis.N Engl J Med. 2012 Feb 2;366(5):474; author reply 475-6. doi: 10.1056/NEJMc1113986. N Engl J Med. 2012. PMID: 22296084 No abstract available.
References
-
- Sterling TR, Pham PA, Chaisson RE. HIV infection-related tuberculosis: clinical manifestations and treatment. Clin Infect Dis. 2010;50 Suppl 3:S223–S230. - PubMed
-
- Burman W, Weis S, Vernon A, et al. Frequency, severity and duration of immune reconstitution events in HIV-related tuberculosis. Int J Tuberc Lung Dis. 2007;11(12):1282–1289. - PubMed
-
- Global Tuberculosis Control: A short update to the 2009 report. 2009 (Accessed at http://whqlibdoc.who.int/publications/2009/9789241598866_eng.pdf)
Publication types
MeSH terms
Substances
Associated data
Grants and funding
- AI68634/AI/NIAID NIH HHS/United States
- 5U01A1069438/PHS HHS/United States
- U01 A169414-03/PHS HHS/United States
- A1069428/PHS HHS/United States
- 5U01A1066453-04/PHS HHS/United States
- U01-A1069501/PHS HHS/United States
- U01 A1069436/PHS HHS/United States
- 5U01A1069417-04/PHS HHS/United States
- 1U01A1069518-01/PHS HHS/United States
- 5U01 A1069455/PHS HHS/United States
- P30 AI027763/AI/NIAID NIH HHS/United States
- U01A1069432/PHS HHS/United States
- U01 AI038855/AI/NIAID NIH HHS/United States
- 5 U01 A1069399-0/PHS HHS/United States
- U011069476-04/PHS HHS/United States
- A1069456/PHS HHS/United States
- A169426/PHS HHS/United States
- K24 AI051982/AI/NIAID NIH HHS/United States
- U01 AI038858/AI/NIAID NIH HHS/United States
- U01 AI068636/AI/NIAID NIH HHS/United States
- U01A1069518/PHS HHS/United States
- AI38838/AI/NIAID NIH HHS/United States
- UM1 AI069496/AI/NIAID NIH HHS/United States
- AI 69432/AI/NIAID NIH HHS/United States
- U01 A1069421/PHS HHS/United States
- 5U01 A1069502/PHS HHS/United States
- 3U01 A1069401/PHS HHS/United States
- U01A1068636/PHS HHS/United States
- A1069463/PHS HHS/United States
- U01 A169469/PHS HHS/United States
- U01 AI068634/AI/NIAID NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials