

Correlation between radiological assessment of acute ankle fractures and syndesmotic injury on MRI
- PMID: 22012479
- PMCID: PMC3368108
- DOI: 10.1007/s00256-011-1284-2
Correlation between radiological assessment of acute ankle fractures and syndesmotic injury on MRI
Abstract
Objective: Owing to the shortcomings of clinical examination and radiographs, injury to the syndesmotic ligaments is often misdiagnosed. When there is no indication requiring that the fractured ankle be operated on, the syndesmosis is not tested intra-operatively, and rupture of this ligamentous complex may be missed. Subsequently the patient is not treated properly leading to chronic complaints such as instability, pain, and swelling. We evaluated three fracture classification methods and radiographic measurements with respect to syndesmotic injury.
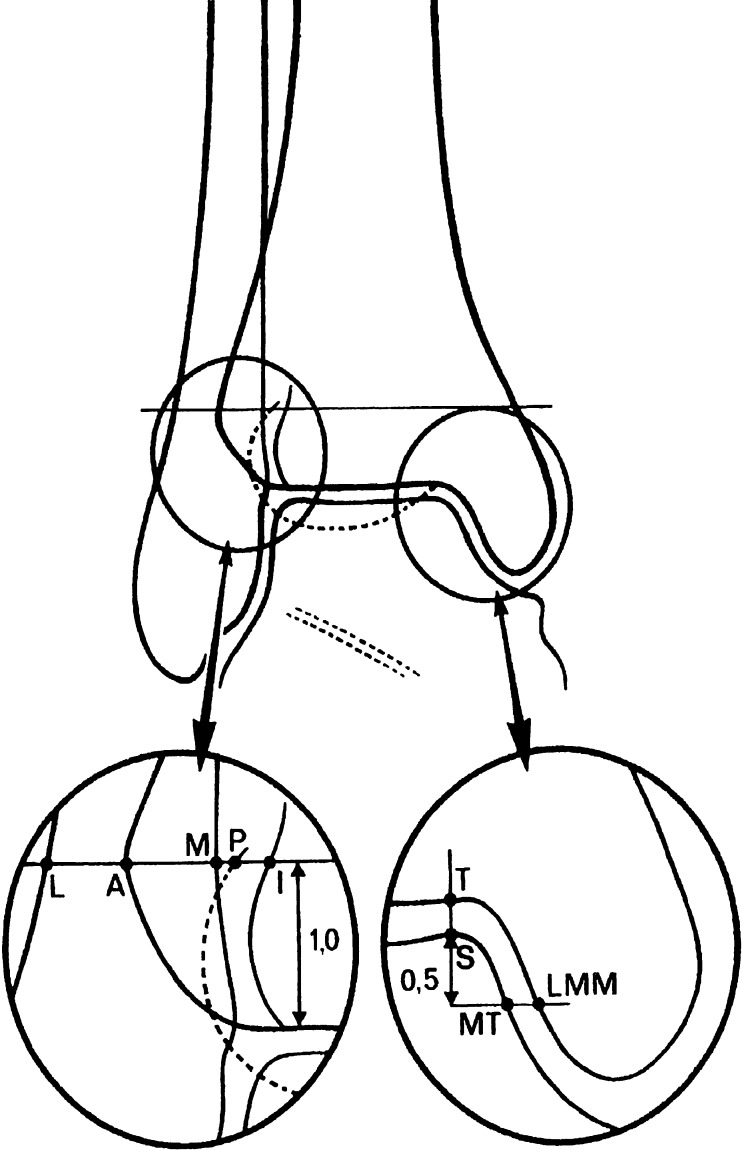
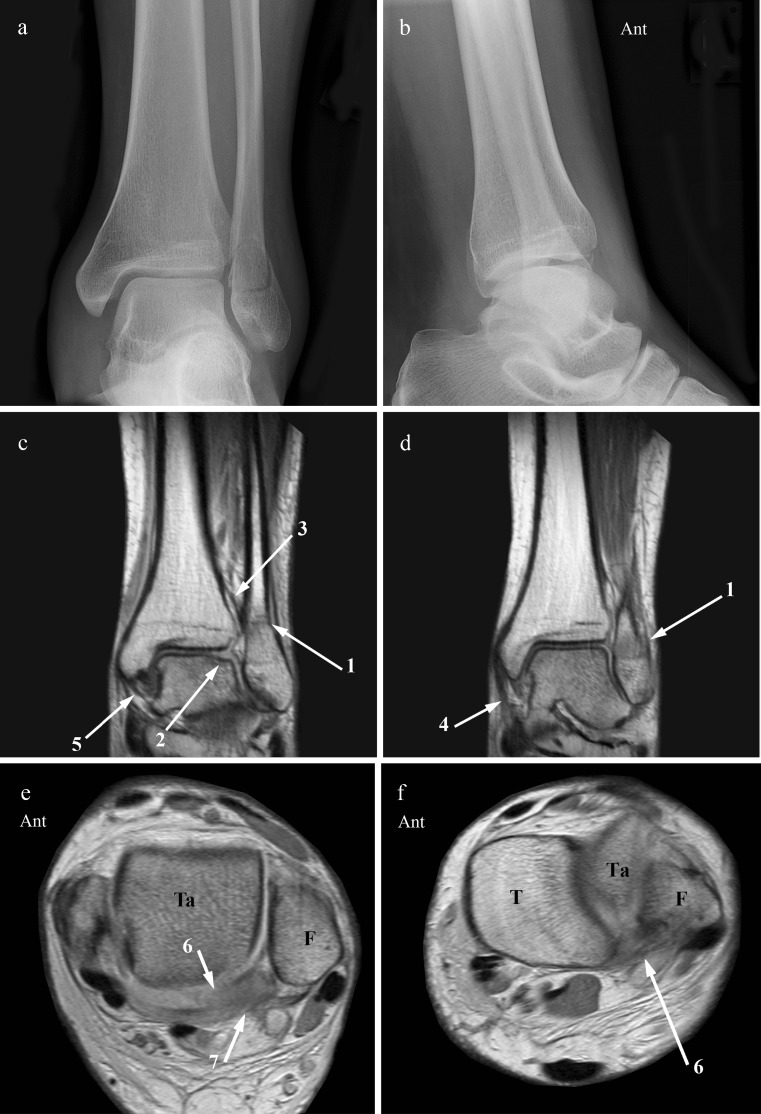
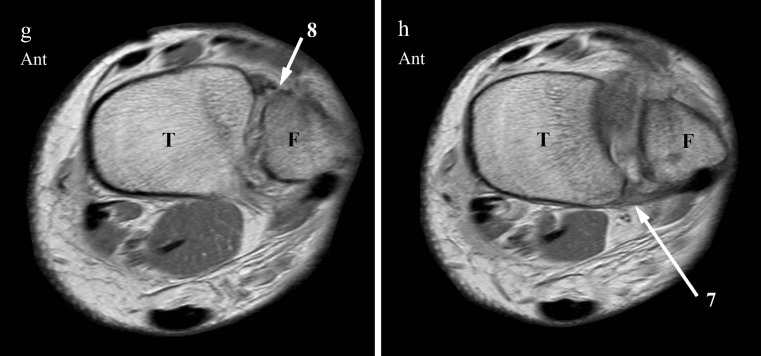
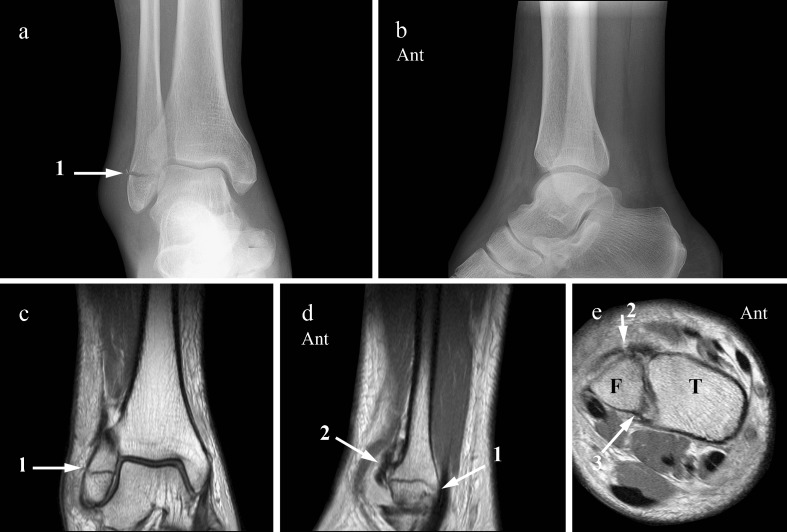
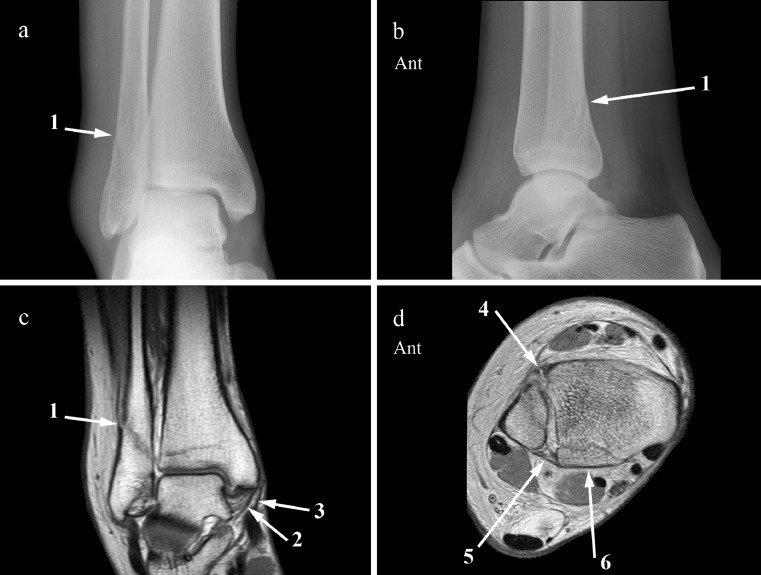
Materials and methods: Prospectively the radiographs of 51 consecutive ankle fractures were classified according to Weber, AO-Müller, and Lauge-Hansen. Both the fracture type and additional measurements of the tibiofibular clear space (TFCS), tibiofibular overlap (TFO), medial clear space (MCS), and superior clear space (SCS) were used to assess syndesmotic injury. MRI, as standard of reference, was performed to evaluate the integrity of the distal tibiofibular syndesmosis. The sensitivity and specificity for detection of syndesmotic injury with radiography were compared to MRI.
Results: The Weber and AO-Müller fracture classification system, in combination with additional measurements, detected syndesmotic injury with a sensitivity of 47% and a specificity of 100%, and Lauge-Hansen with both a sensitivity and a specificity of 92%. TFCS and TFO did not correlate with syndesmotic injury, and a widened MCS did not correlate with deltoid ligament injury.
Conclusion: Syndesmotic injury as predicted by the Lauge-Hansen fracture classification correlated well with MRI findings. With MRI the extent of syndesmotic injury and therefore fracture stage can be assessed more accurately compared to radiographs.
Figures


References
-
- Kelikian H, Kelikian S. Disorders of the ankle. London: W.B. Saunders Company; 1985.
-
- Kapandji IA. Funktionelle Anatomie der Gelenke. Schematisierte und kommentierte Zeichnungen zur menslichen Biomechanik. Stuttgart: Ferdinand Enke; 1985. 148–65.
-
- Lutz W. Zur Struktur der unteren Tibiofibularverbindung und der Membrana interossea cruris. Anat Entwickl Gesch. 1942;111:315–321. doi: 10.1007/BF00538090. - DOI
-
- Weber BG. Die Verletzungen des oberen Sprunggelenkes. Zweite, überarbeitete und ergänzte Auflage. Vienna: Hans Huber Bern Stuttgart; 1972.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
