

Design of a randomized trial of diabetes genetic risk testing to motivate behavior change: the Genetic Counseling/lifestyle Change (GC/LC) Study for Diabetes Prevention
- PMID: 22013171
- PMCID: PMC3763721
- DOI: 10.1177/1740774511414159
Design of a randomized trial of diabetes genetic risk testing to motivate behavior change: the Genetic Counseling/lifestyle Change (GC/LC) Study for Diabetes Prevention
Abstract
Background: The efficacy of diabetes genetic risk testing to motivate behavior change for diabetes prevention is currently unknown.
Purpose: This paper presents key issues in the design and implementation of one of the first randomized trials (The Genetic Counseling/Lifestyle Change (GC/LC) Study for Diabetes Prevention) to test whether knowledge of diabetes genetic risk can motivate patients to adopt healthier behaviors.
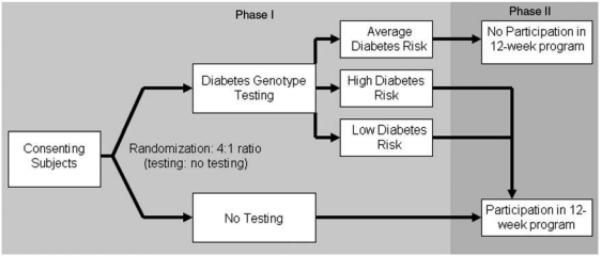
Methods: Because individuals may react differently to receiving 'higher' vs 'lower' genetic risk results, we designed a 3-arm parallel group study to separately test the hypotheses that: (1) patients receiving 'higher' diabetes genetic risk results will increase healthy behaviors compared to untested controls, and (2) patients receiving 'lower' diabetes genetic risk results will decrease healthy behaviors compared to untested controls. In this paper we describe several challenges to implementing this study, including: (1) the application of a novel diabetes risk score derived from genetic epidemiology studies to a clinical population, (2) the use of the principle of Mendelian randomization to efficiently exclude 'average' diabetes genetic risk patients from the intervention, and (3) the development of a diabetes genetic risk counseling intervention that maintained the ethical need to motivate behavior change in both 'higher' and 'lower' diabetes genetic risk result recipients.
Results: Diabetes genetic risk scores were developed by aggregating the results of 36 diabetes-associated single nucleotide polymorphisms. Relative risk for type 2 diabetes was calculated using Framingham Offspring Study outcomes, grouped by quartiles into 'higher', 'average' (middle two quartiles) and 'lower' genetic risk. From these relative risks, revised absolute risks were estimated using the overall absolute risk for the study group. For study efficiency, we excluded all patients receiving 'average' diabetes risk results from the subsequent intervention. This post-randomization allocation strategy was justified because genotype represents a random allocation of parental alleles ('Mendelian randomization'). Finally, because it would be unethical to discourage participants to participate in diabetes prevention behaviors, we designed our two diabetes genetic risk counseling interventions (for 'higher' and 'lower' result recipients) so that both groups would be motivated despite receiving opposing results.
Limitations: For this initial assessment of the clinical implementation of genetic risk testing we assessed intermediate outcomes of attendance at a 12-week diabetes prevention course and changes in self-reported motivation. If effective, longer term studies with larger sample sizes will be needed to assess whether knowledge of diabetes genetic risk can help patients prevent diabetes.
Conclusions: We designed a randomized clinical trial designed to explore the motivational impact of disclosing both higher than average and lower than average genetic risk for type 2 diabetes. This design allowed exploration of both increased risk and false reassurance, and has implications for future studies in translational genomics.
Figures
References
-
- Kaprio J, Tuomilehto J, Koskenvuo M, et al. Concordance for type 1 (insulin-dependent) and type 2 6 RW Grant et al. Clinical Trials. 2011;00:1–7.
- diabetes mellitus in a population-based cohort of twins in Finland. Diabetologia. 1992;35:1060–7. http://ctj.sagepub.com(non-insulin-dependent) - PubMed
-
- Durbin RM, Abecasis GR, Altshuler DL, et al. 1000 Genomes Project C. Nature. 2010;467:1061–73.
-
- McBride CM, Koehly LM, Sanderson SC, Kaphingst KA. The behavioral response to personalized genetic information: Will genetic risk profiles motivate individuals and families to choose more healthful behaviors? Annu Rev Public Health. 2010;31:89–103. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
