Dexmedetomidine attenuates sympathoadrenal response to tracheal intubation and reduces perioperative anaesthetic requirement
- PMID: 22013250
- PMCID: PMC3190508
- DOI: 10.4103/0019-5049.84846
Dexmedetomidine attenuates sympathoadrenal response to tracheal intubation and reduces perioperative anaesthetic requirement
Abstract
Background: Dexmedetomidine, an α-2 adrenoreceptor agonist, is gaining popularity for its sympatholytic, sedative, anaesthetic sparing and haemodynamic stabilising properties without significant respiratory depression.
Methods: We assessed the efficacy of dexmedetomidine in attenuating sympathoadrenal response to tracheal intubation and analysed reduction in intraoperative anaesthetic requirement. Sixty patients scheduled for elective surgery of more than 3 hours were randomly selected. Control group received isoflurane-opioid and study group received isoflurane-opioid-dexmedetomidine anaesthesia. Dexmedetomidine infusion in a dose of 1 μg/kg was given over 10 min before the induction of anaesthesia and was continued in a dose of 0.2-0.7 μg/kg/Hr until skin closure. All patients were induced with thiopentone, fentanyl and vecuronium. Haemodynamic variables were continuously recorded.
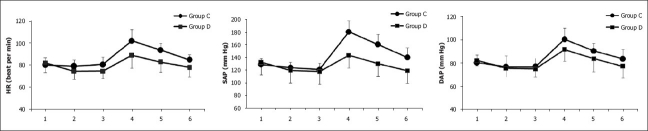
Results: The need for thiopentone and isoflurane was decreased by 30% and 32%, respectively, in the dexmedetomidine group as compared to the control group. After tracheal intubation, maximal average increase was 8% in systolic and 11% in diastolic blood pressure in dexmedetomidine group, as compared to 40% and 25%, respectively, in the control group. Similarly, average increase in heart rate was 7% and 21% in the dexmedetomidine and control groups, respectively. Fentanyl requirement during the operation was 100±10 μg in the control group and 60±10 μg in the dexmedetomidine group.
Conclusion: Perioperative infusion of dexmedetomidine is effective in attenuating sympathoadrenal response to tracheal intubation. It has significant anaesthetic and opioid sparing effect.
Keywords: dexmedetomidine; sympathoadrenal response; tracheal intubation; α-2 adrenoreceptor.
Conflict of interest statement
Figures
References
-
- Bloor BC, Flacke WE. Reduction in halothane anesthetic requirement by clonidine: An α adrenergic agonist. Anesth Analg. 1982;61:741–5. - PubMed
-
- Ghignone M, Quintin L, Duke PC, Kehler CH, Cavillo O. Effects of clonidine on narcotic requirements and hemodynamic responses during induction of fentanyl anesthesia and endotracheal intubation. Anesthesiology. 1986;64:36–42. - PubMed
-
- Flacke JW, Bloor BC, Flacke WE, Wong D, Dazza S, Stead W, et al. Reduced narcotic requirement by clonidine with improved hemodynamic and adrenergic stability in patients undergoing coronary bypass surgery. Anesthesiology. 1987;67:11–9. - PubMed
-
- Pottu J, Scheinin B, Rosenberg PH, Viinamaki O, Scheinin M. Oral premedication with clonidine: Effects on stress response during general anesthesia. Acta Anaesthesiol Scand. 1987;31:730–4. - PubMed
-
- Savola JM, Ruskoaho H, Puurunen J, Salonen JS, Karki NT. Evidence for medetomidine as a selective and potent agonist at α2-adrenoreceptors. J Autonomic Pharmacol. 1986;5:275–84. - PubMed