

Association of CD14+ monocyte-derived progenitor cells with cardiac allograft vasculopathy
- PMID: 22014346
- PMCID: PMC3202640
- DOI: 10.1016/j.jtcvs.2011.07.032
Association of CD14+ monocyte-derived progenitor cells with cardiac allograft vasculopathy
Abstract
Objective: The pathogenesis of cardiac allograft vasculopathy after heart transplant remains controversial. Histologically, cardiac allograft vasculopathy is characterized by intimal hyperplasia of the coronary arteries induced by infiltrating cells. The origin of these infiltrating cells in cardiac allograft vasculopathy is unclear. Endothelial progenitor cells are reportedly involved in cardiac allograft vasculopathy; however, the role of CD14(+) monocyte-derived progenitor cells in cardiac allograft vasculopathy pathogenesis remains unknown.
Methods: Monocyte-derived progenitor cells were isolated from blood mononuclear cell fractions obtained from 25 patients with cardiac allograft vasculopathy and 25 patients without cardiac allograft vasculopathy.
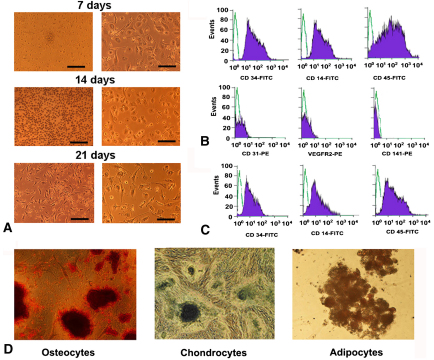
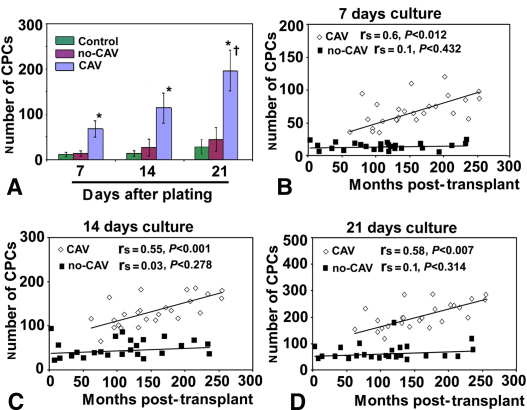
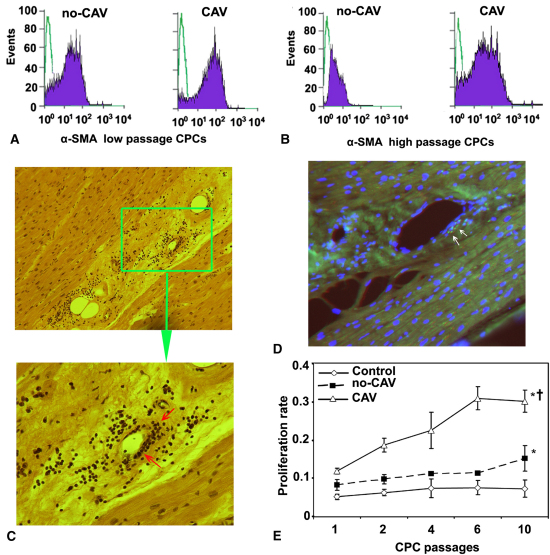
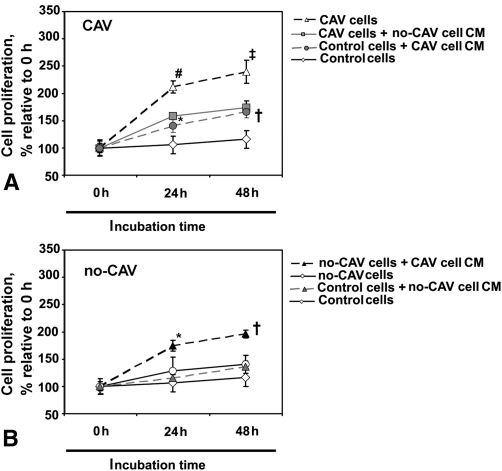
Results: Both patients with cardiac allograft vasculopathy and those without cardiac allograft vasculopathy had CD45(+), CD34(+), CD14(+), CD141(-), CD31(-) monocyte-derived progenitor cells that differentiated into mesenchymal lineages. Monocyte-derived progenitor cells formed significantly higher numbers of colonies in patients with cardiac allograft vasculopathy than in those without cardiac allograft vasculopathy; this correlated with posttransplant follow-up time. Importantly, monocyte-derived progenitor cells from patients with cardiac allograft vasculopathy expressed significantly more α smooth muscle actin and proliferated at a higher rate than did monocyte-derived progenitor cells of patients without cardiac allograft vasculopathy. In vitro experiments suggested a paracrine control mechanism in proliferation of monocyte-derived progenitor cells in cardiac allograft vasculopathy.
Conclusions: These results indicate that monocyte-derived progenitor cells are associated with cardiac allograft vasculopathy, have the ability to transdifferentiate into smooth muscle cells, and thus may contribute to intimal hyperplasia of coronary arteries in cardiac allograft vasculopathy. Targeting monocyte-derived progenitor cell recruitment could be beneficial in cardiac allograft vasculopathy treatment.
Copyright © 2011 The American Association for Thoracic Surgery. Published by Mosby, Inc. All rights reserved.
Figures
References
-
- Taylor D.O., Stehlik J., Edwards L.B., Aurora P., Christie J.D., Dobbels F. Registry of the International Society for Heart and Lung Transplantation: twenty-sixth official adult heart transplantation report—2009. J Heart Lung Transplant. 2009;28:1007–1022. - PubMed
-
- Valantine H. Cardiac allograft vasculopathy after heart transplantation: risk factors and management. J Heart Lung Transplant. 2004;23(5 Suppl):187–193. - PubMed
-
- Mitchell R.N., Libby P. Vascular remodeling in transplant vasculopathy. Circ Res. 2007;100:967–978. - PubMed
-
- Waller J., Brook N.R., Nicholson M.L. Cardiac allograft vasculopathy: current concepts and treatment. Transpl Int. 2003;16:367–375. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
