

Lateral and syndesmotic ankle sprain injuries: a narrative literature review
- PMID: 22014912
- PMCID: PMC3259913
- DOI: 10.1016/j.jcm.2011.02.001
Lateral and syndesmotic ankle sprain injuries: a narrative literature review
Abstract
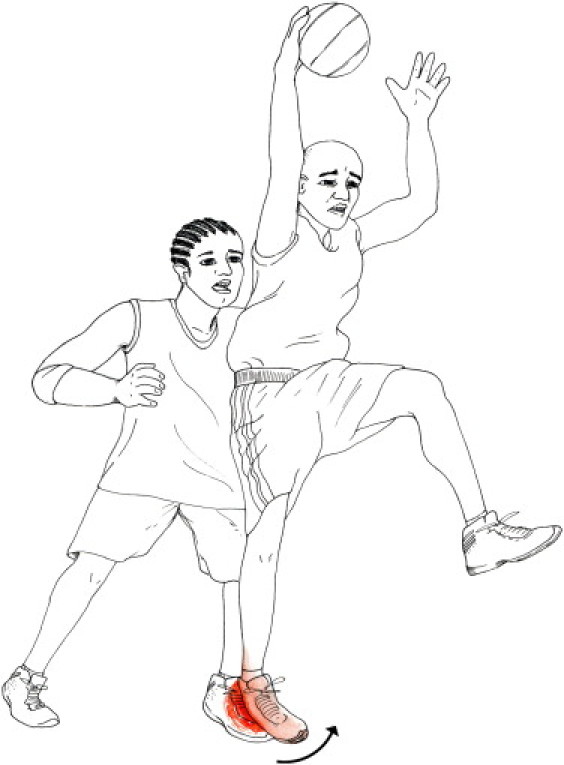
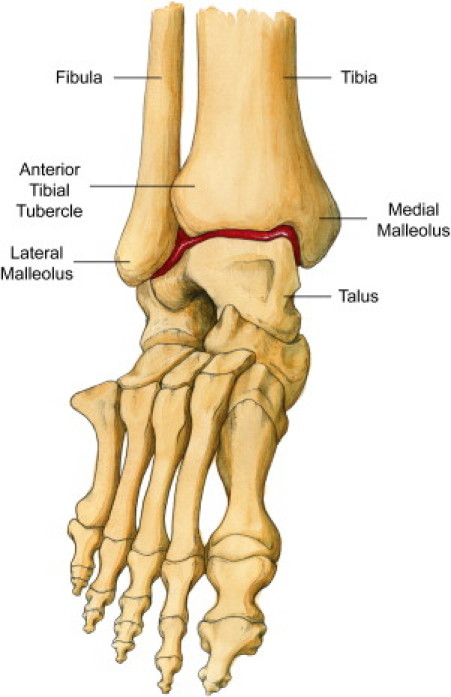
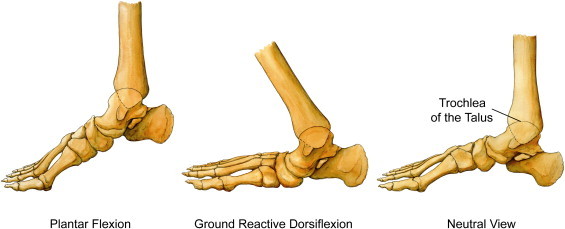
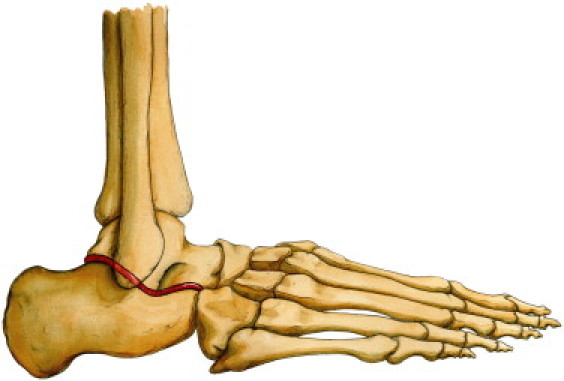
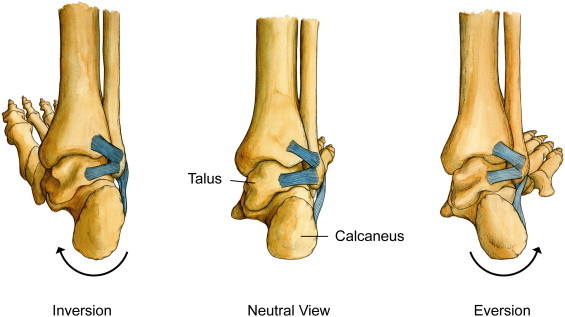
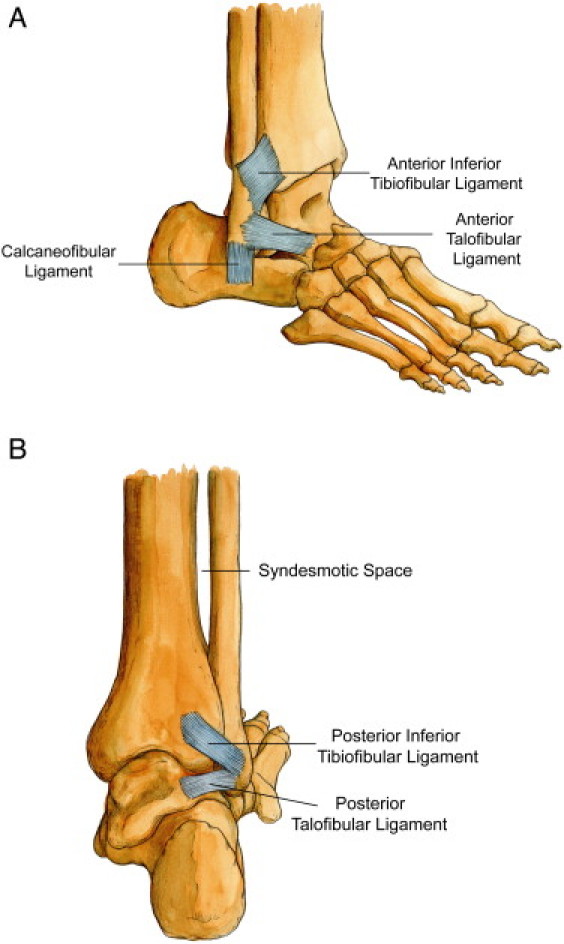
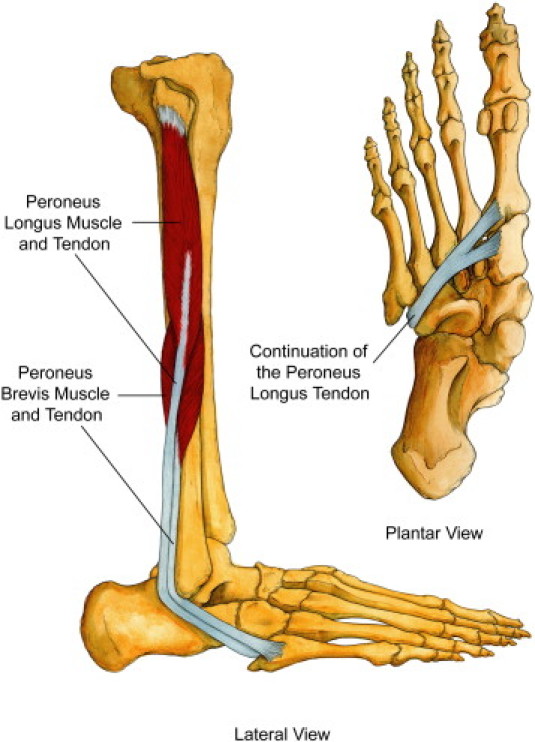
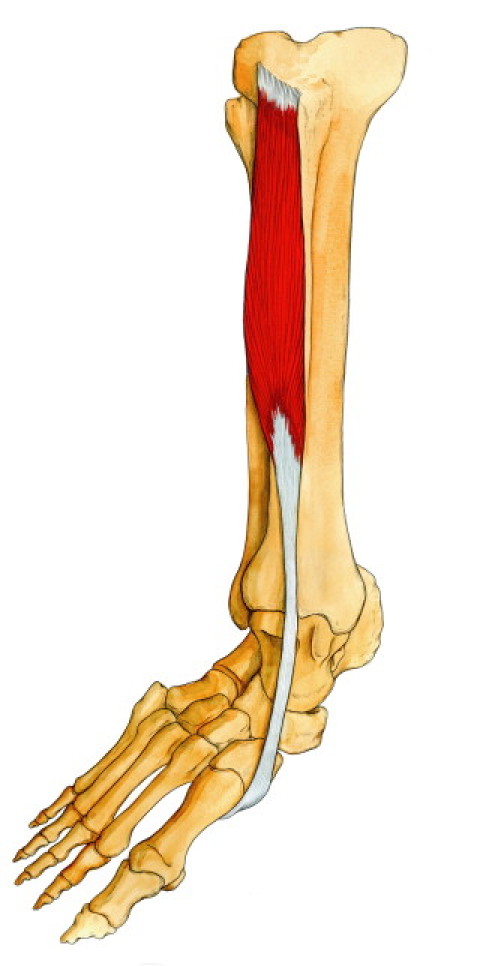
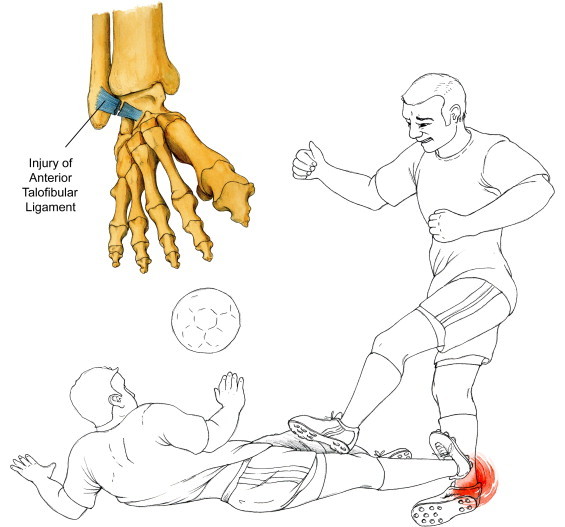
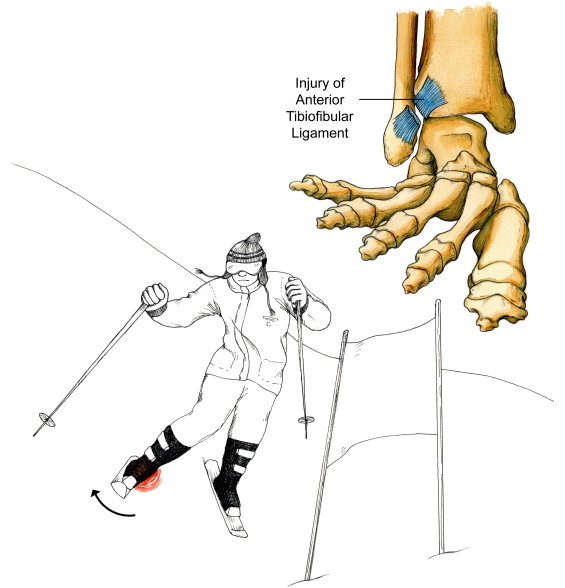
Objective: The purpose of this article is to review the literature that discusses normal anatomy and biomechanics of the foot and ankle, mechanisms that may result in a lateral ankle sprain or syndesmotic sprain, and assessment and diagnostic procedures, and to present a treatment algorithm based on normal ligament healing principles.
Methods: Literature was searched for years 2000 to 2010 in PubMed and CINAHL. Key search terms were ankle sprain$, ankle injury and ankle injuries, inversion injury, proprioception, rehabilitation, physical therapy, anterior talofibular ligament, syndesmosis, syndesmotic injury, and ligament healing.
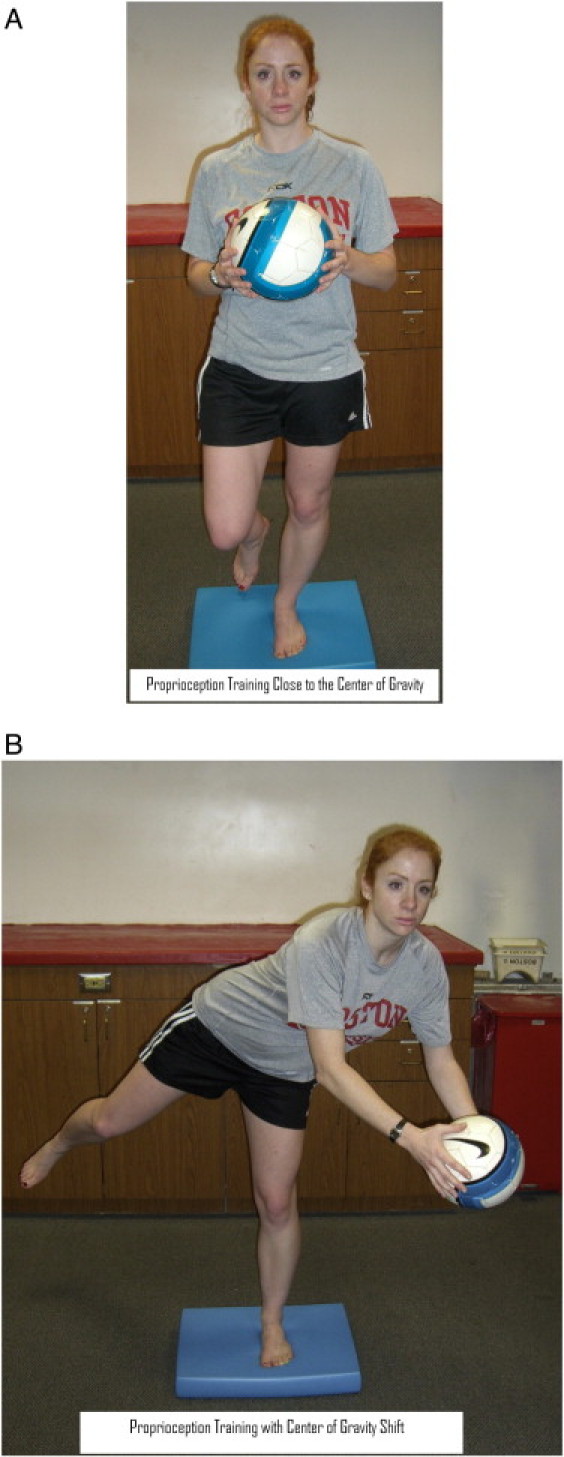
Discussion: Most ankle sprains respond favorably to nonsurgical treatment, such as those offered by physical therapists, doctors of chiropractic, and rehabilitation specialists. A comprehensive history and examination aid in diagnosing the severity and type of ankle sprain. Based on the diagnosis and an understanding of ligament healing properties, a progressive treatment regimen can be developed. During the acute inflammatory phase, the goal of care is to reduce inflammation and pain and to protect the ligament from further injury. During the reparative and remodeling phase, the goal is to progress the rehabilitation appropriately to facilitate healing and restore the mechanical strength and proprioception. Radiographic imaging techniques may need to be used to rule out fractures, complete ligament tears, or instability of the ankle mortise. A period of immobilization and ambulating with crutches in a nonweightbearing gait may be necessary to allow for proper ligament healing before commencing a more active treatment approach. Surgery should be considered in the case of grade 3 syndesmotic sprain injuries or those ankle sprains that are recalcitrant to conservative care.
Conclusion: An accurate diagnosis and prompt treatment can minimize an athlete's time lost from sport and prevent future reinjury. Most ankle sprains can be successfully managed using a nonsurgical approach.
Copyright © 2011 National University of Health Sciences. Published by Elsevier Inc. All rights reserved.
Figures
References
-
- Safran M.R., Bendetti R.S., Bartolozzi A.R., III, Mandelbaum B.R. Lateral ankle sprains: a comprehensive review part 1: etiology, pathoanatomy, histopathogenesis, and diagnosis. Med Sci Sports. 1999;31(7):S429–S437. - PubMed
-
- Reid D.C. Sports injury assessment and rehabilitation. Churchill Livingston Inc.; New York: 1992. pp. 215–268.
-
- Wester J.U., Jespersen S.M., Nielsen K.D., Neumann L. Wobble board training after partial sprains of the lateral ligaments of the ankle: a prospective randomized study. J Orthop Sports Phys Ther. 1996;23(5):332–336. - PubMed
-
- Munn J., Beard D., Refshauge K.M., Lee R.Y.W. Eccentric muscle strength in functional ankle instability. Med Sci Sports. 2003;35(2):245–250. - PubMed
-
- Beynnon B.D., Vacek P.M., Murphy D., Alosa D., Paller D. First time inversion ankle ligament trauma. Am J Sports Med. 2005;33(10):1485–1491. - PubMed
LinkOut - more resources
Full Text Sources
