

Pulmonary artery and intestinal temperatures during heat stress and cooling
- PMID: 22015711
- PMCID: PMC3289717
- DOI: 10.1249/MSS.0b013e31823d7a2b
Pulmonary artery and intestinal temperatures during heat stress and cooling
Abstract
Purpose: In humans, whole body heating and cooling are used to address physiological questions where core temperature is central to the investigated hypotheses. Core temperature can be measured in various locations throughout the human body. The measurement of intestinal temperature is increasingly used in laboratory settings as well as in athletics. However, it is unknown whether intestinal temperature accurately tracks pulmonary artery blood temperature, the gold standard, during thermal stimuli in resting humans, which is the investigated hypothesis.
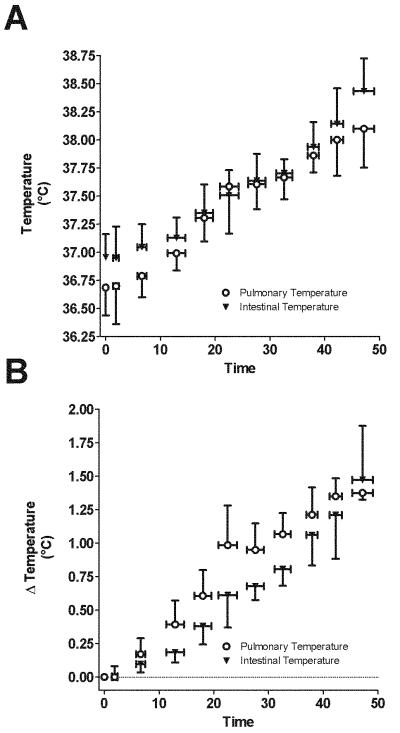
Methods: This study compared pulmonary artery blood temperature (via thermistor in a pulmonary artery catheter) with intestinal temperature (telemetry pill) during whole body heat stress (n = 8), followed by whole body cooling in healthy humans (mean ± SD; age = 24 ± 3 yr, height = 183 ± 8 cm, mass = 78.1 ± 8.2 kg). Heat stress and subsequent cooling were performed by perfusing warm followed by cold water through a tube-lined suit worn by each subject.
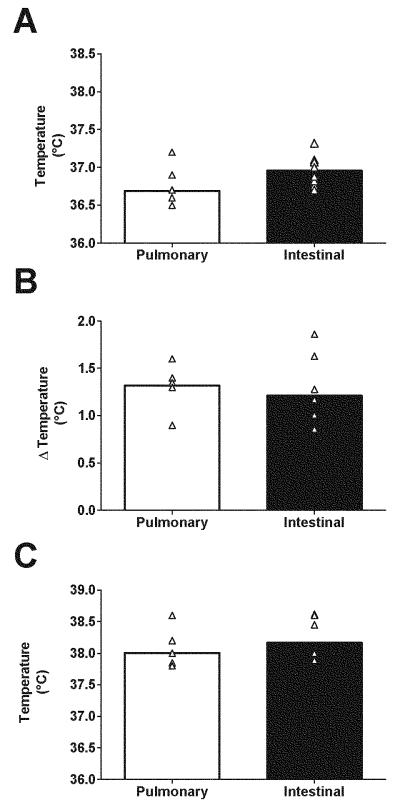
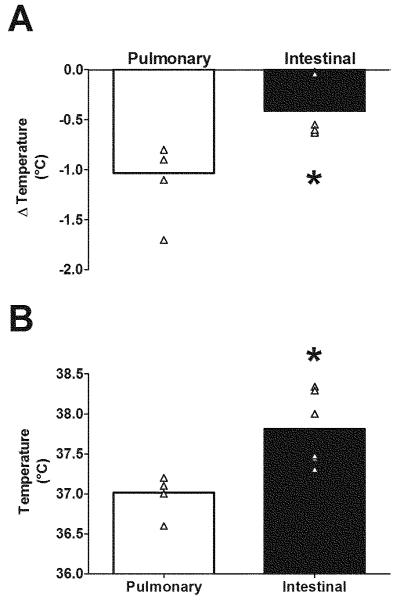
Results: Before heat stress, blood temperature (36.69°C ± 0.25°C) was less than intestinal temperature (36.96°C ± 0.21°C, P = 0.004). The increase in blood temperature after 20 min of heat stress was greater than the intestinal temperature (0.70 ± 0.24 vs 0.47 ± 0.18, P = 0.001). However, the increase in temperatures at the end of heat stress was similar between sites (blood Δ = 1.32°C ± 0.20°C vs intestinal Δ = 1.21°C ± 0.36°C, P = 0.30). Subsequent cooling decreased blood temperature (Δ = -1.03°C ± 0.34°C) to a greater extent than intestinal temperature (Δ = -0.41°C ± 0.30°C, P = 0.04).
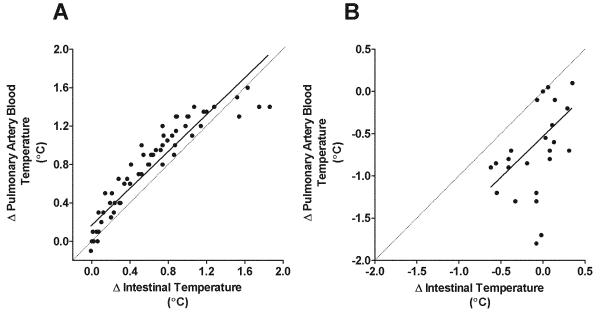
Conclusions: In response to the applied thermal provocations, early temperature changes in the intestine are less than the temperature changes in pulmonary artery blood.
Figures
References
-
- Armstrong LE, Casa DJ, Millard-Stafford M, Moran DS, Pyne SW, Roberts WO. American College of Sports Medicine position stand. Exertional heat illness during training and competition. Med Sci Sports Exerc. 2007;39(3):556–72. - PubMed
-
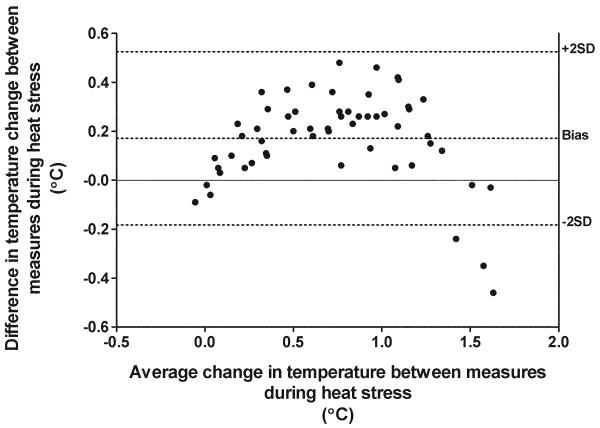
- Bland JM, Altman DG. Statistical methods for assessing agreement between two methods of clinical measurement. Lancet. 1986;1(8476):307–10. - PubMed
-
- Bligh J. Temperature regulation in mammals and other vertebrates. North-Holland; London: 1973. pp. 80–84.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
