

Effect of regional anesthesia on the success rate of external cephalic version: a systematic review and meta-analysis
- PMID: 22015882
- PMCID: PMC3199126
- DOI: 10.1097/AOG.0b013e3182324583
Effect of regional anesthesia on the success rate of external cephalic version: a systematic review and meta-analysis
Abstract
Objective: To estimate whether the use of regional anesthesia is associated with increased success of external cephalic version.
Data sources: We searched MEDLINE, EMBASE, the Cochrane Library, and clinical trial registries.
Methods of study selection: Electronic databases were searched from 1966 through April 2011 for published, randomized controlled trials in the English language comparing regional anesthesia with no regional anesthesia for external cephalic version. The primary outcome was external cephalic version success. Secondary outcomes included cesarean delivery, maternal discomfort, and adverse events. Pooled risk ratios (relative risk) were calculated using a random-effects model. Heterogeneity was assessed using the Cochran's Q statistic and quantified using the I Z method.
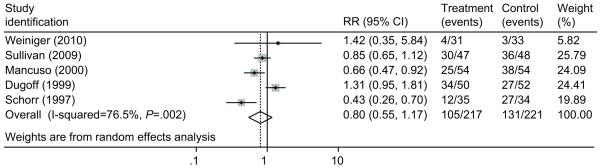
Tabulation, integration, and results: Six randomized controlled trials met criteria for study inclusion. Regional anesthesia was associated with a higher external cephalic version success rate compared with intravenous or no analgesia (59.7% compared with 37.6%; pooled relative risk 1.58; 95% confidence interval [CI] 1.29-1.93). This significant association persisted when the data were stratified by type of regional anesthesia (spinal compared with epidural). The number needed to treat with regional anesthesia to achieve one additional successful external cephalic version was five. There was no evidence of statistical heterogeneity (P=.32, I Z=14.9%) or publication bias (Harbord test P=.78). There was no statistically significant difference in the risk of cesarean delivery comparing regional anesthesia with intravenous or no analgesia (48.4% compared with 59.3%; pooled relative risk 0.80; 95% CI 0.55-1.17). Adverse events were rare and not significantly different between the two groups.
Conclusion: Regional anesthesia is associated with a higher success rate of external cephalic version.
Figures



Similar articles
-
Neuraxial analgesia to increase the success rate of external cephalic version: a systematic review and meta-analysis of randomized controlled trials.Am J Obstet Gynecol. 2016 Sep;215(3):276-86. doi: 10.1016/j.ajog.2016.04.036. Epub 2016 Apr 27. Am J Obstet Gynecol. 2016. PMID: 27131581
-
Venous cutdown versus the Seldinger technique for placement of totally implantable venous access ports.Cochrane Database Syst Rev. 2016 Aug 21;2016(8):CD008942. doi: 10.1002/14651858.CD008942.pub2. Cochrane Database Syst Rev. 2016. PMID: 27544827 Free PMC article.
-
Epidural versus non-epidural or no analgesia for pain management in labour.Cochrane Database Syst Rev. 2018 May 21;5(5):CD000331. doi: 10.1002/14651858.CD000331.pub4. Cochrane Database Syst Rev. 2018. PMID: 29781504 Free PMC article.
-
Interventions for helping to turn term breech babies to head first presentation when using external cephalic version.Cochrane Database Syst Rev. 2012 Jan 18;1:CD000184. doi: 10.1002/14651858.CD000184.pub3. Cochrane Database Syst Rev. 2012. Update in: Cochrane Database Syst Rev. 2015 Feb 09;(2):CD000184. doi: 10.1002/14651858.CD000184.pub4. PMID: 22258940 Free PMC article. Updated.
-
Antioxidants for female subfertility.Cochrane Database Syst Rev. 2017 Jul 28;7(7):CD007807. doi: 10.1002/14651858.CD007807.pub3. Cochrane Database Syst Rev. 2017. Update in: Cochrane Database Syst Rev. 2020 Aug 27;8:CD007807. doi: 10.1002/14651858.CD007807.pub4. PMID: 28752910 Free PMC article. Updated.
Cited by
-
A randomized trial of remifentanil for analgesia in external cephalic version for breech presentation.Medicine (Baltimore). 2016 Dec;95(49):e5483. doi: 10.1097/MD.0000000000005483. Medicine (Baltimore). 2016. PMID: 27930530 Free PMC article. Clinical Trial.
-
Exploring fetal growth patterns in the second trimester: insights from ultrasound measurements among the Minangkabau Ethnic Group in Indonesia.BMC Pregnancy Childbirth. 2025 Jan 24;25(1):68. doi: 10.1186/s12884-024-07042-5. BMC Pregnancy Childbirth. 2025. PMID: 39856642 Free PMC article.
-
Effect of anesthesia on the success rate of external cephalic version: GRADE- assessed systematic review and meta-analysis of randomized controlled trials.Syst Rev. 2024 Jul 30;13(1):202. doi: 10.1186/s13643-024-02616-y. Syst Rev. 2024. PMID: 39080805 Free PMC article.
-
Coming out ahead: the cost effectiveness of external cephalic version using spinal anesthesia.Isr J Health Policy Res. 2014 Feb 24;3(1):6. doi: 10.1186/2045-4015-3-6. Isr J Health Policy Res. 2014. PMID: 24565024 Free PMC article.
-
Neuraxial block and success of external cephalic version.BJA Educ. 2020 Sep;20(9):296-297. doi: 10.1016/j.bjae.2020.05.001. Epub 2020 Jul 18. BJA Educ. 2020. PMID: 33456963 Free PMC article. No abstract available.
References
-
- American College of Obstetricians and Gynecologists . Practice Bulletin #13: External Cephalic Version. American College of Obstetricians and Gynecologists; Washington D.C.: 2000.
-
- Hannah ME, Hannah WJ, Hewson SA, Hodnett ED, Saigal S, Willan AR, Term Breech Trial Collaborative Group Planned caesarean section versus planned vaginal birth for breech presentation at term: a randomized multicentre trial. Lancet. 2000;356:1375–1383. - PubMed
-
- American College of Obstetricians and Gynecologists . Mode of term singleton breech delivery. American College of Obstetricians and Gynecologists; Washington D.C.: 2006. Committee Opinion #340.
-
- Kok M, van der Steeg JW, van der Post JA, Mol BW. Prediction of success of external cephalic version after 36 weeks. Am J Perinatol. 2011;28:103–110. - PubMed
-
- Burgos J, Melchor JC, Pijoan JI, Cobos P, Fernandez-Llebrez L, Martinez-Astorquiza T. A prospective study of the factors associated with the success rate of external cephalic version for breech presentation at term. Int J Gynaecol Obstet. 2011;112:48–51. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
