

Neurogenic changes in the upper airway of patients with obstructive sleep apnea
- PMID: 22016445
- PMCID: PMC3297112
- DOI: 10.1164/rccm.201106-1058OC
Neurogenic changes in the upper airway of patients with obstructive sleep apnea
Abstract
Rationale: Controversy persists regarding the presence and importance of hypoglossal nerve dysfunction in obstructive sleep apnea (OSA).
Objectives: We assessed quantitative parameters related to motor unit potential (MUP) morphology derived from electromyographic (EMG) signals in patients with OSA versus control subjects and hypothesized that signs of neurogenic remodeling would be present in the patients with OSA.
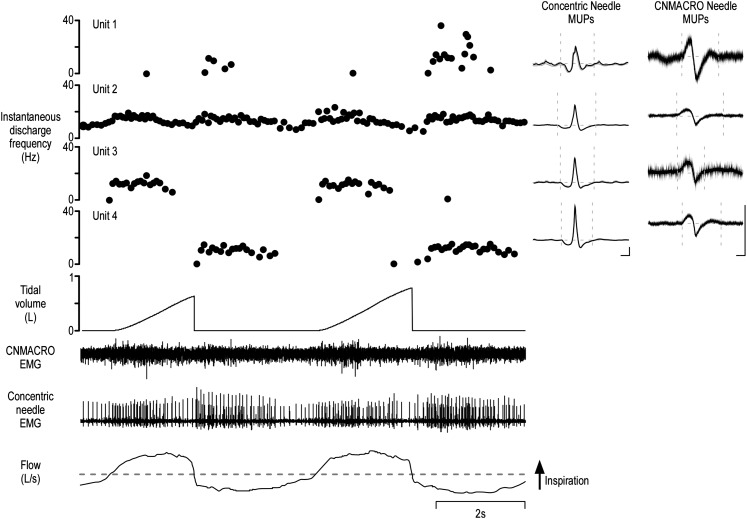
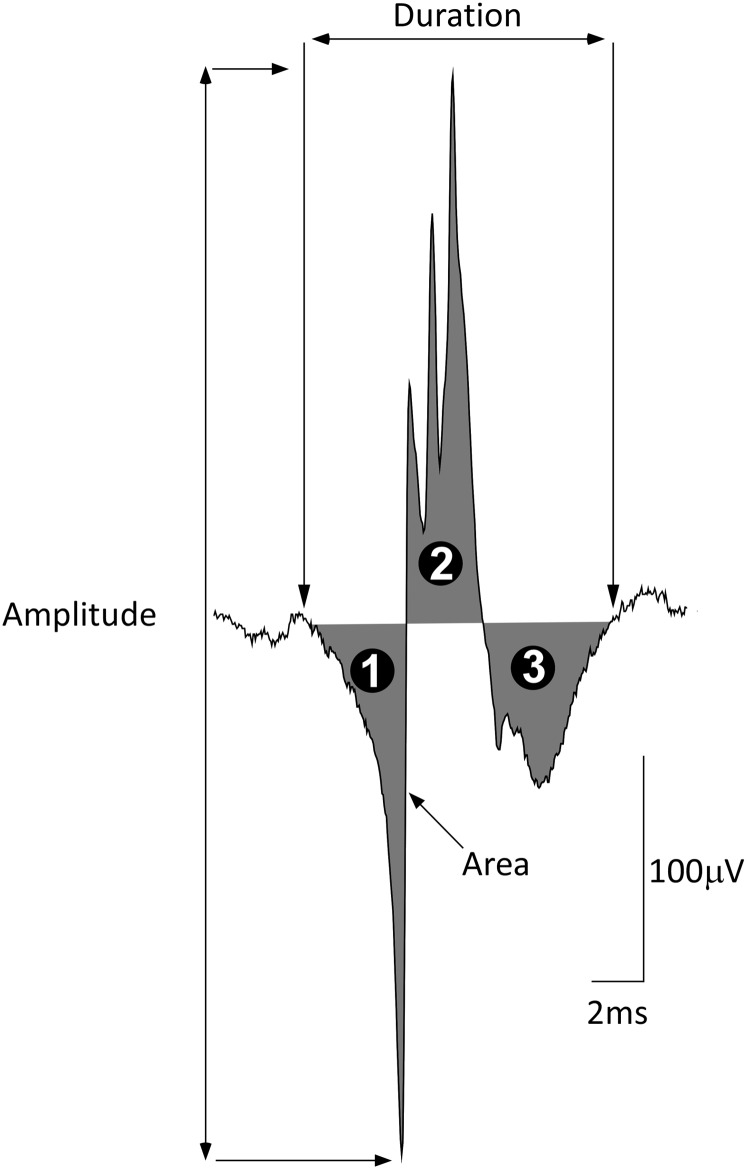
Methods: Participants underwent diagnostic sleep studies to obtain apnea-hypopnea indices. Muscle activity was detected with 50-mm concentric needle electrodes. The concentric needle was positioned at more than 10 independent sites per subject, after the local anatomy of the upper airway musculature was examined by ultrasonography. All activity was quantified with subjects awake, during supine eupneic breathing while wearing a nasal mask connected to a pneumotachograph. Genioglossus EMG signals were analyzed offline by automated software (DQEMG), which extracted motor unit potential trains (MUPTs) contributed by individual motor units from the composite EMG signals. Quantitative measurements of MUP templates, including duration, peak-to-peak amplitude, area, area-to-amplitude ratio, and size index, were compared between the untreated patients with OSA and healthy control subjects.
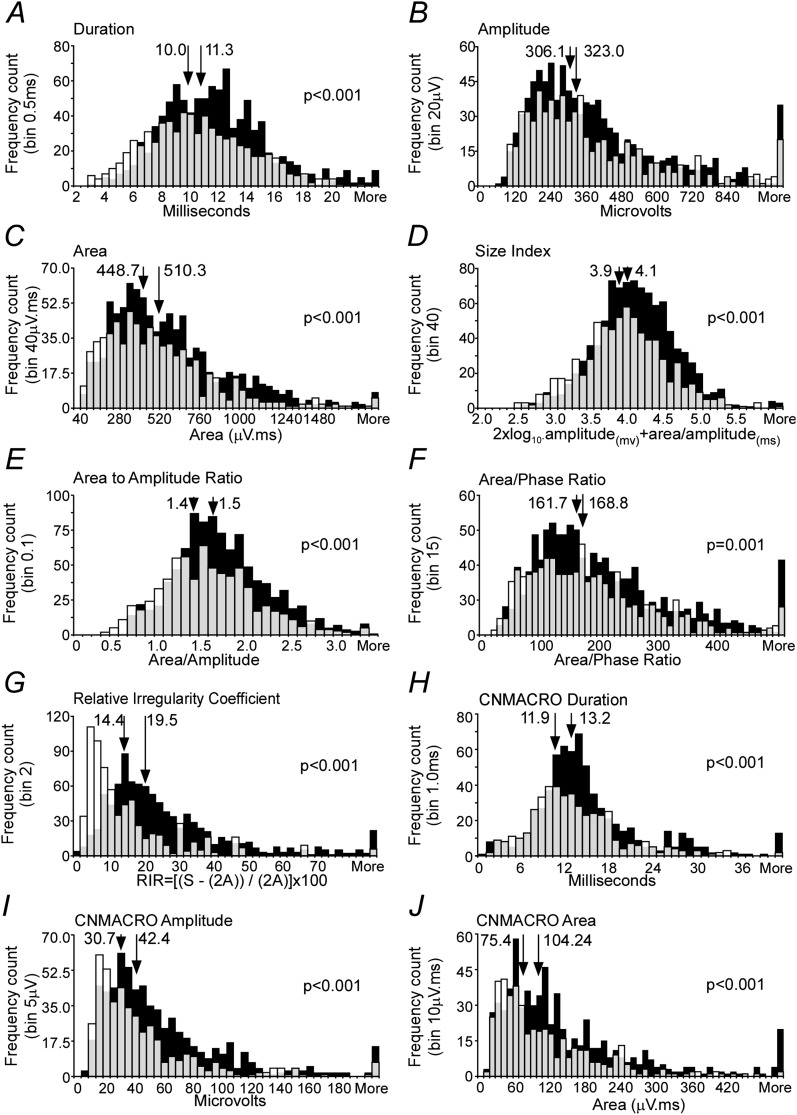
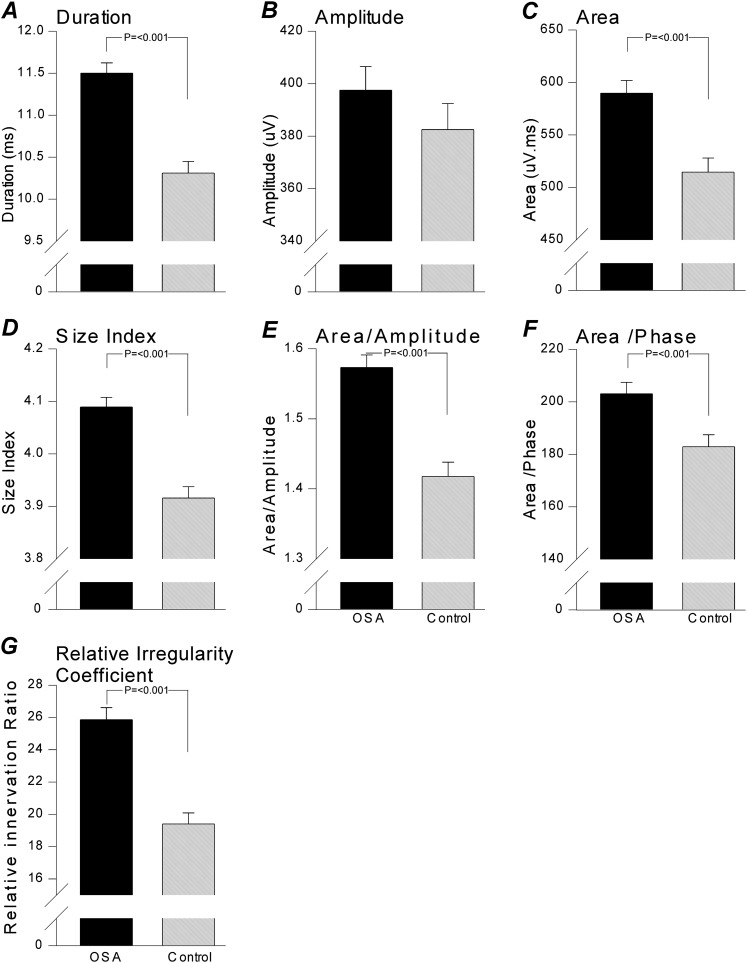
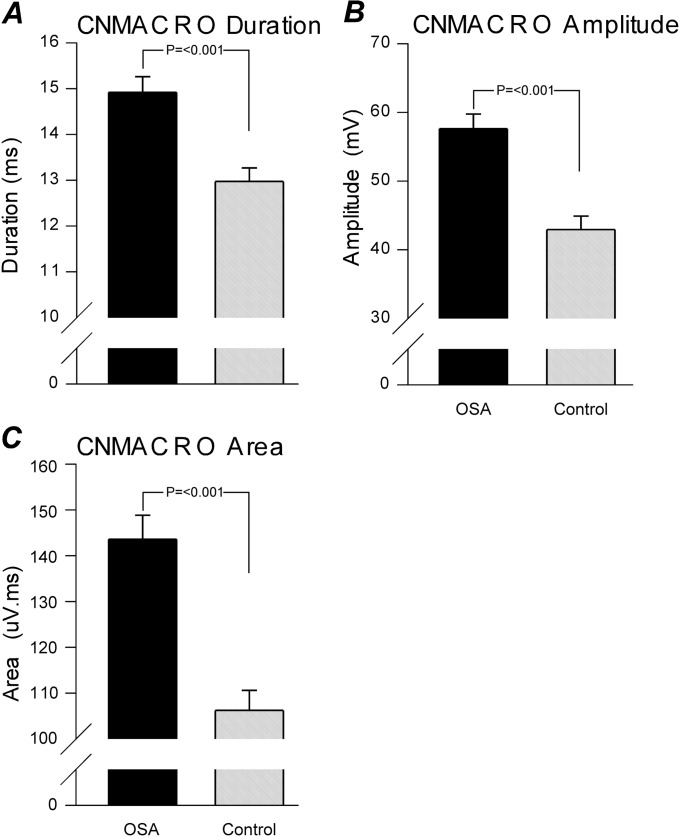
Measurements and main results: A total of 1,655 MUPTs from patients with OSA (n = 17; AHI, 55 ± 6/h) and control subjects (n = 14; AHI, 4 ± 1/h) were extracted from the genioglossus muscle EMG signals. MUP peak-to-peak amplitudes in the patients with OSA were not different compared with the control subjects (397.5 ± 9.0 vs. 382.5 ± 10.0 μV). However, the MUPs of the patients with OSA were longer in duration (11.5 ± 0.1 vs. 10.3 ± 0.1 ms; P < 0.001) and had a larger size index (4.09 ± 0.02 vs. 3.92 ± 0.02; P < 0.001) compared with control subjects.
Conclusions: These results confirm and quantify the extent and existence of structural neural remodeling in OSA.
Figures
Comment in
-
Pharyngeal neuropathy in obstructive sleep apnea: where are we going?Am J Respir Crit Care Med. 2012 Feb 1;185(3):241-3. doi: 10.1164/rccm.201111-1992ED. Am J Respir Crit Care Med. 2012. PMID: 22298363 No abstract available.
References
-
- Kimoff RJ, Sforza E, Champagne V, Ofiara L, Gendron D. Upper airway sensation in snoring and obstructive sleep apnea. Am J Respir Crit Care Med 2001;164:250–255 - PubMed
-
- Nguyen AT, Jobin V, Payne R, Beauregard J, Naor N, Kimoff RJ. Laryngeal and velopharyngeal sensory impairment in obstructive sleep apnea. Sleep 2005;28:585–593 - PubMed
-
- Friberg D. Heavy snorer's disease: a progressive local neuropathy. Acta Otolaryngol 1999;119:925–933 - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
