

Peripheral blood proteins predict mortality in idiopathic pulmonary fibrosis
- PMID: 22016448
- PMCID: PMC3262037
- DOI: 10.1164/rccm.201101-0058OC
Peripheral blood proteins predict mortality in idiopathic pulmonary fibrosis
Erratum in
- Am J Respir Crit Care Med. 2012 Feb 15;185(4):464
Abstract
Rationale: Idiopathic pulmonary fibrosis (IPF) is a lethal lung disease of unknown etiology with a variable and unpredictable course.
Objectives: The aim of this study was to identify and validate plasma proteins that are predictive of outcome in IPF.
Methods: Plasma samples were available for 241 patients with IPF (140 derivation and 101 validation). In the derivation cohort, concentrations of 92 proteins were analyzed using a multiplex bead-based immunoassay and concentrations of matrix metalloproteinase (MMP)-7, MMP-1, and surfactant protein D were assessed by ELISA. In the validation cohort concentrations of intercellular adhesion molecule (ICAM)-1, IL-8, and vascular cell adhesion molecule (VCAM)-1 were assessed by bead-based multiplex assay, and S100A12 and MMP-7 by ELISA. Associations of biomarkers with mortality, transplant-free survival, and disease progression were tested in the derivation and validation cohorts using nonparametric methods of survival analysis and the Cox proportional hazards model, and an integrated risk prediction score was derived and tested.
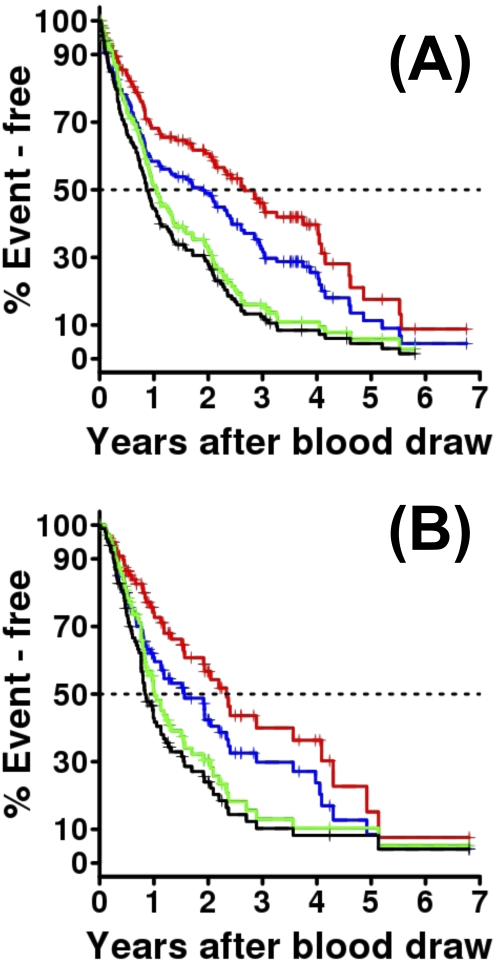
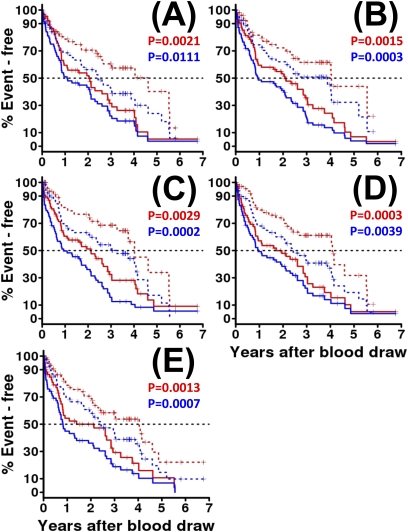
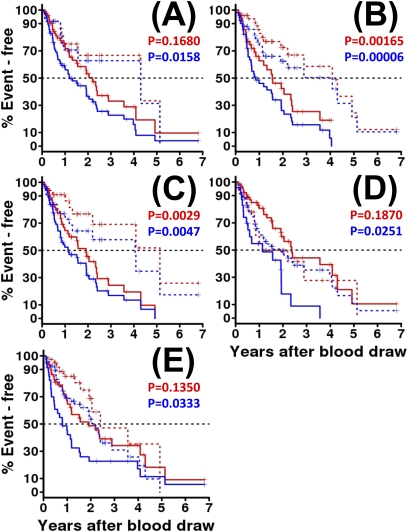
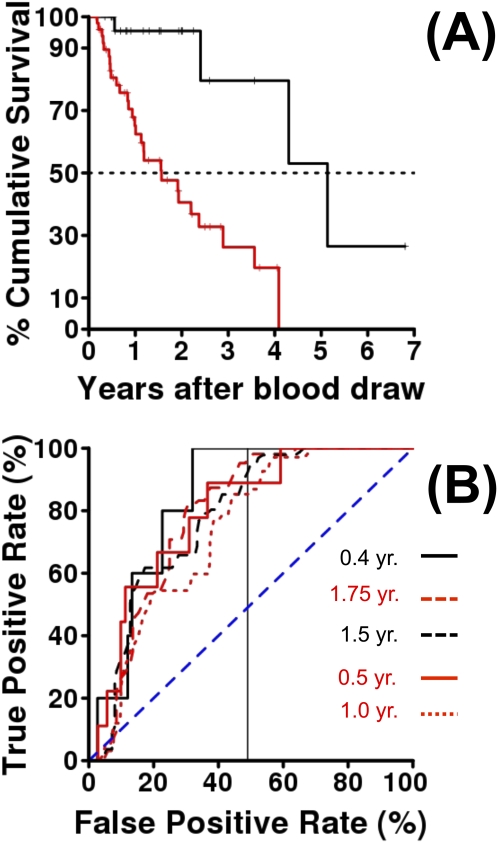
Measurements and main results: High concentrations of MMP-7, ICAM-1, IL-8, VCAM-1, and S100A12 predicted poor overall survival, poor transplant-free survival, and poor progression-free survival in the derivation cohort. In the independent validation cohort high concentrations of all five were predictive of poor transplant-free survival; MMP-7, ICAM-1, and IL-8 of overall survival; and ICAM-1 of poor progression-free survival. The personal clinical and molecular mortality prediction index derived in the derivation cohort was highly predictive of mortality in the validation cohort.
Conclusions: Our results suggest that plasma proteins should be evaluated as a tool for prognosis determination in prioritization of patients for lung transplantation and stratification in drug studies.
Figures
Comment in
-
Risk prediction in idiopathic pulmonary fibrosis.Am J Respir Crit Care Med. 2012 Jan 1;185(1):6-7. doi: 10.1164/rccm.201111-1960ED. Am J Respir Crit Care Med. 2012. PMID: 22210784 No abstract available.
References
-
- Strieter RM. Pathogenesis and natural history of usual interstitial pneumonia: the whole story or the last chapter of a long novel. Chest 2005;128:526S–532S - PubMed
-
- Selman M, King TE, Pardo A. Idiopathic pulmonary fibrosis: prevailing and evolving hypotheses about its pathogenesis and implications for therapy. Ann Intern Med 2001;134:136–151 - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous
