

Burden of new and recurrent tuberculosis in a major South African city stratified by age and HIV-status
- PMID: 22016763
- PMCID: PMC3189963
- DOI: 10.1371/journal.pone.0025098
Burden of new and recurrent tuberculosis in a major South African city stratified by age and HIV-status
Abstract
Aim: To describe the burden of tuberculosis (TB) in Cape Town by calculating TB incidence rates stratified by age and HIV-status, assessing the contribution of retreatment disease and estimating the cumulative lifetime TB risk in HIV-negative individuals.
Methods: Details of TB cases were abstracted from the 2009 electronic TB register. Population denominators were estimated from census data and actuarial estimates of HIV prevalence, allowing calculation of age-specific and HIV-stratified TB notification rates.
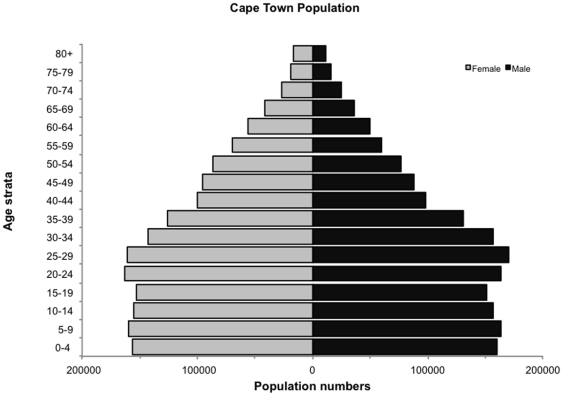
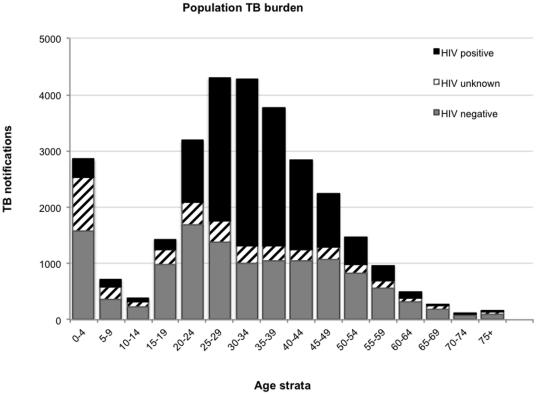
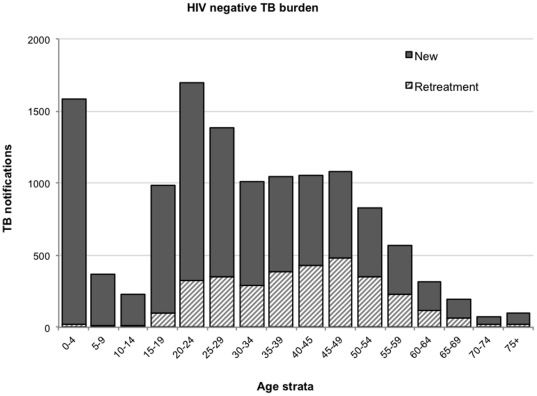
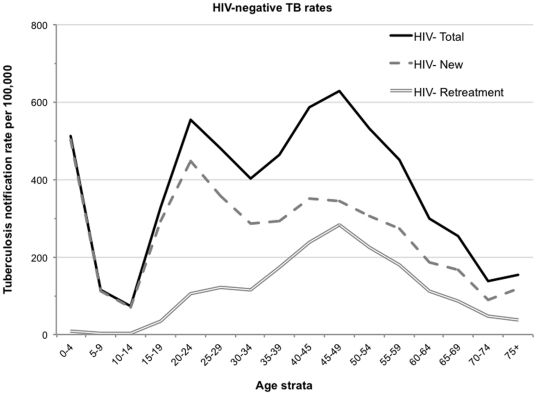
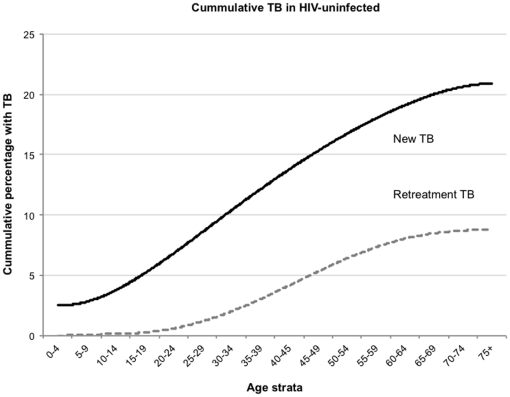
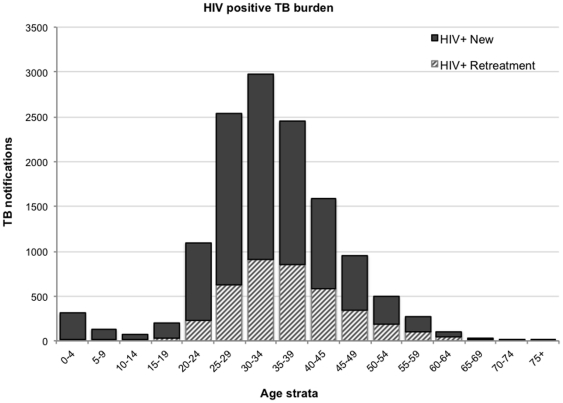
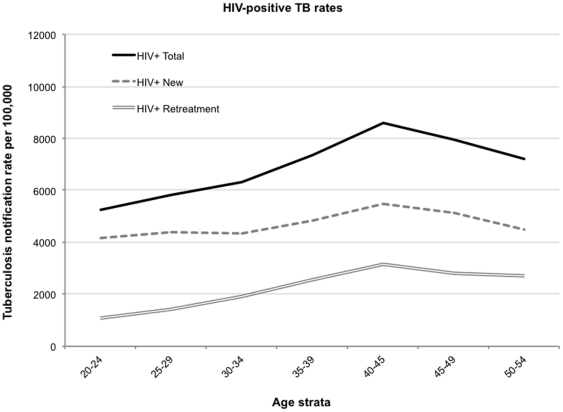
Results: The 2009 mid-year population was 3,443,010 (3,241,508 HIV-negative and 201,502 HIV-positive individuals). There were 29,478 newly notified TB cases of which 56% were laboratory confirmed. HIV status was recorded for 87% of cases and of those with known HIV-status 49% were HIV-negative and 51% were positive. Discrete peaks in the incidence of non-HIV-associated TB occurred at three ages: 511/100,000 at 0-4 years of age, 553/100,000 at 20-24 years and 628/100,000 at 45-49 years with 1.5%, 19% and 45% being due to retreatment TB, respectively. Only 15.5% of recurrent cases had a history of TB treatment failure or default. The cumulative lifetime risks in the HIV-negative population of all new TB episodes and new smear-positive TB episodes were 24% and 12%, respectively; the lifetime risk of retreatment disease was 9%. The HIV-positive notification rate was 6,567/100,000 (HIV-associated TB rate ratio = 17). Although retreatment cases comprised 30% of the HIV-associated TB burden, 88% of these patients had no history of prior treatment failure or default.
Conclusions: The annual burden of TB in this city is huge. TB in the HIV-negative population contributed almost half of the overall disease burden and cumulative lifetime risks were similar to those reported in the pre-chemotherapy era. Retreatment TB contributed significantly to both HIV-associated and non-HIV-associated TB but infrequently followed prior inadequate treatment. This likely reflects ongoing TB transmission to both HIV-negative and positive individuals.
Conflict of interest statement
Figures
References
-
- World Health Organization. Global tuberculosis control. World Health Organization, Geneva.; 2009. Epidemiology, strategy, financing. WHO/HTM/TB/2009.411 Accessible at the following URL: http://www.who.int/tb/publications/global_report/2009/en/index.html. Accessed 1st March 2011.
-
- World Health Organization. Global tuberculosis control. A short update to the 2009 report. WHO, Geneva, 2009.; 2009. Accessible at the following URL: http://www.who.int/tb/publications/global_report/2009/update/tbu9.pdf Accessed 1st March 2011.
-
- Cape Town TB Control - Progress Report 1997-2003 Available at URL http://www.hst.org.za/publications/618 Accessed 1st March 2011.
-
- Lawn SD, Bekker LG, Middelkoop K, Myer L, Wood R. Impact of HIV on epidemiology of tuberculosis in a peri-urban community in South Africa: the need for age-specific interventions. Clin Infect Dis. 2006;42:1040–1047]. - PubMed
-
- The South African Tuberculosis Control Programme. Practical Guidelines 2000; Available at URL http://www.doh.gov.za/tb/index.html Accessed 1st March 2011. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
