

Ionizing radiation induces neuroendocrine differentiation of prostate cancer cells in vitro, in vivo and in prostate cancer patients
- PMID: 22016831
- PMCID: PMC3196282
Ionizing radiation induces neuroendocrine differentiation of prostate cancer cells in vitro, in vivo and in prostate cancer patients
Abstract
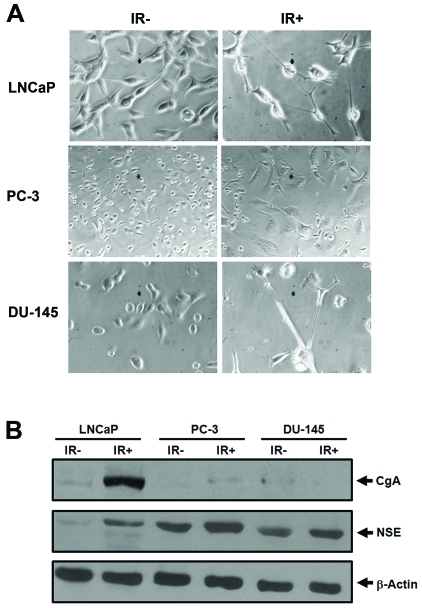
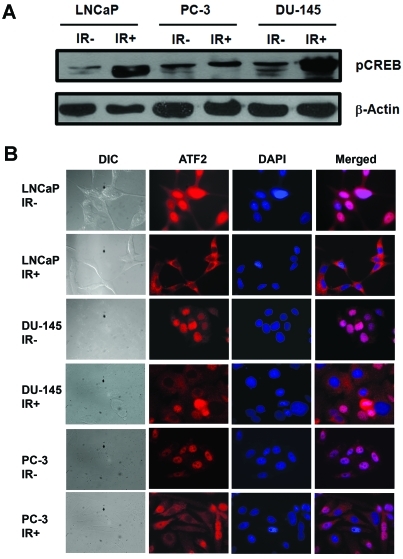
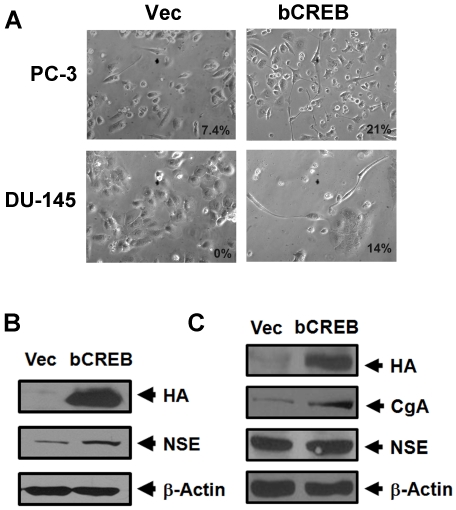
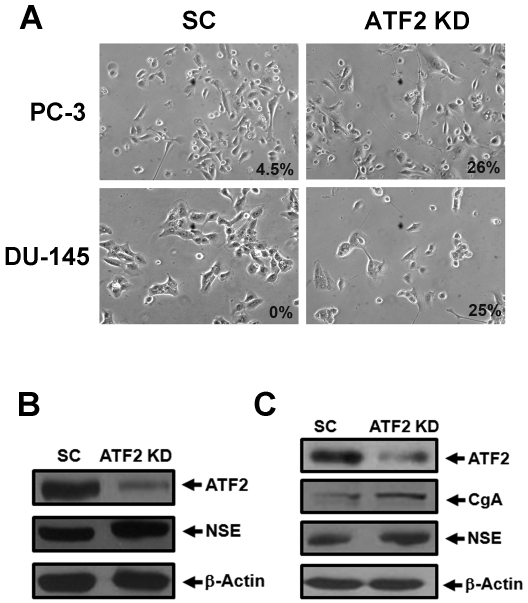
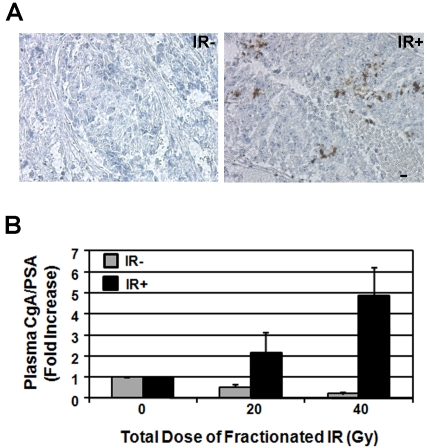
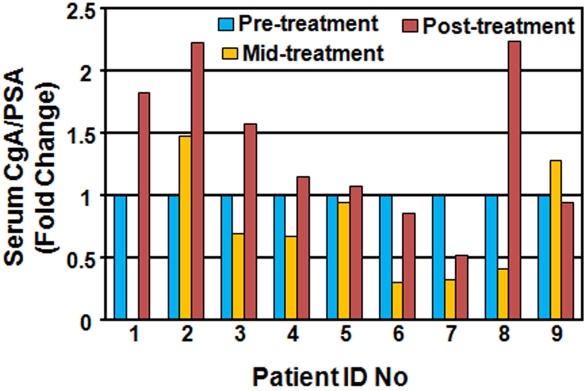
Prostate cancer remains the most common noncutaneous cancer among American men. Although most patients can be cured by surgery and radiotherapy, 32,050 patients still died of the disease in 2010. Many patients receive radiotherapy either as a primary therapy, salvage therapy, or in combination with surgery or hormonal therapy. Despite initial treatment, several studies suggest that approximately 10% of low-risk prostate cancer patients and up to 30-60% with more advanced cancer patients experience biochemical recurrence within five years after radiotherapy. Thus, elucidating the molecular mechanisms underlying radioresistance and tumor recurrence has the potential to significantly reduce prostate cancer mortality. We previously demonstrated that fractionated ionizing radiation (IR) can induce the prostate cancer cell line LNCaP to undergo neuroendocrine differentiation (NED) by activation of cAMP response element binding protein (CREB) and cytoplasmic sequestration of ATF2, two CRE-binding transcription factors that oppose each other to regulate NED. Importantly, IR-induced NED is reversible and de-differentiated cells are cross-resistant to IR, androgen depletion and docetaxel treatments. These findings suggest that radiation-induced NED may allow prostate cancer cells to survive treatment and contribute to tumor recurrence. In the present study, we further demonstrated that IR also induces NED in a subset of DU-145 and PC-3 cells. In addition, we confirmed that IR induces NED in LNCaP xenograft tumors in nude mice, and observed that the plasma chro-mogranin A (CgA) level, a biomarker for NED, is increased by 2- to 5-fold in tumor-bearing mice after fractionated radiation doses of 20 and 40 Gy, respectively. Consistent with these in vivo findings, a pilot study in prostate cancer patients showed that the serum CgA level is elevated in 4 out of 9 patients after radiotherapy. Taken together, these findings provide evidence that radiation-induced NED is a general therapeutic response in a subset of prostate cancer patients. Thus, a large scale analysis of radiotherapy-induced NED in prostate cancer patients and its correlation to clinical outcomes will likely provide new insight into the role of NED in prostate cancer radiotherapy and prognosis.
Keywords: ATF2; CREB; Ionizing radiation; neuroendocrine differentiation; prostate cancer; radiotherapy.
Figures
References
-
- Jemal A, Siegel R, Ward E, Hao Y, Xu J, Thun MJ. Cancer statistics, 2009. CA Cancer J Clin. 2009;59:225–49. - PubMed
-
- Kuban DA, Thames HD, Levy LB, Horwitz EM, Kupelian PA, Martinez AA, Michalski JM, Pisansky TM, Sandler HM, Shipley WU, Zelefsky MJ, Zietman AL. Long-term multi-institutional analysis of stage T1-T2 prostate cancer treated with radiotherapy in the PSA era. Int J Radiat Oncol Biol Phys. 2003;57:915–28. - PubMed
-
- Zietman AL, DeSilvio ML, Slater JD, Rossi CJ, Jr, Miller DW, Adams JA, Shipley WU. Comparison of conventional-dose vs high-dose conformal radiation therapy in clinically localized adenocarcinoma of the prostate: a randomized controlled trial. JAMA. 2005;294:1233–9. - PubMed
-
- D'Amico AV, Chen MH, Renshaw AA, Loffredo B, Kantoff PW. Risk of prostate cancer recurrence in men treated with radiation alone or in conjunction with combined or less than combined androgen suppression therapy. J Clin Oncol. 2008;26:2979–83. - PubMed
-
- Agarwal PK, Sadetsky N, Konety BR, Resnick MI, Carroll PR. Treatment failure after primary and salvage therapy for prostate cancer: likelihood, patterns of care, and outcomes. Cancer. 2008;112:307–14. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials