

Hormonal contraception and area of cervical ectopy: a longitudinal assessment
- PMID: 22018127
- PMCID: PMC4262923
- DOI: 10.1016/j.contraception.2011.02.002
Hormonal contraception and area of cervical ectopy: a longitudinal assessment
Abstract
Background: The effect of combined oral contraceptives (COCs) and depot-medroxyprogesterone acetate (DMPA) on the area of cervical ectopy is not well understood.
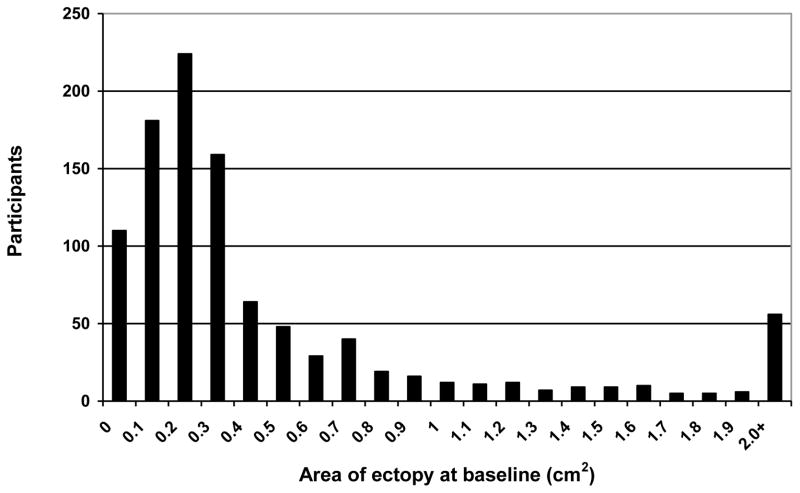
Study design: From 1996 to 1999, we recruited women not using hormonal contraception from two family planning centers in Baltimore, MD. Upon study entry and 3, 6 and 12 months after the initial visit, participants were interviewed and received visual cervical examinations with photography. Ectopy was measured from digitized photographs and was analyzed both continuously and categorically (small [≤0.48 cm(2)] vs. large [>0.48 cm(2)]).
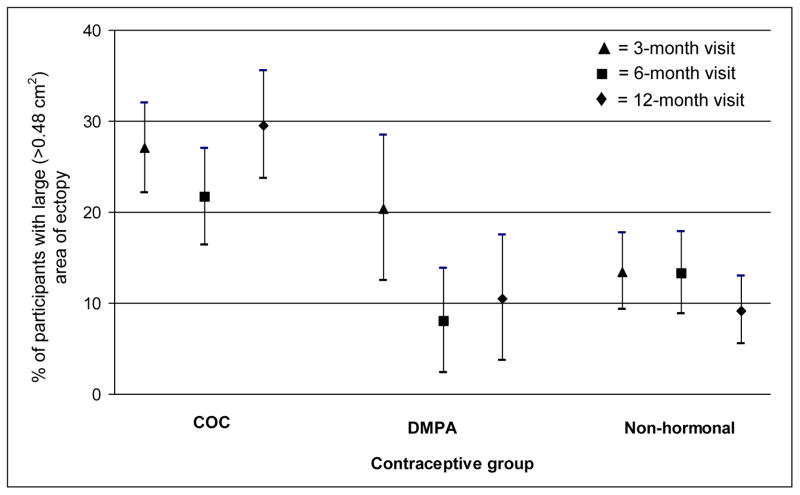
Results: Of 1003 enrolled women, 802 returned for at least one follow-up visit. At 12 months, the numbers of women using COCs, DMPA or no hormonal method at least 50% of the time since the prior visit were 230, 76 and 229, respectively. After multivariable adjustment, COC use (vs. no hormonal use) was associated with large area of ectopy (odds ratio [OR]: 1.8, 95% confidence interval [CI]: 1.0-3.3). No significant relationship was observed between DMPA and large area of ectopy (OR: 0.5, 95% CI: 0.2-1.3). The incidence of large area of ectopy by contraceptive exposure (COC, DMPA or no hormonal method) was 17.4 (CI: 11.8-24.6), 10.9 (CI: 4.4-22.4) and 4.6 (CI: 2.2-8.4) per 100 woman-years, respectively.
Conclusions: Use of COCs, but not DMPA, was associated with large area of cervical ectopy. Area of ectopy at baseline was the strongest predictor of area of ectopy at follow-up.
Copyright © 2011 Elsevier Inc. All rights reserved.
Figures
References
-
- Stamm WE. Chlamydia trachomatis infections of the adult. In: Holmes KK, Sparling PF, Mårdh P, et al., editors. Sexually Transmitted Diseases. 3. New York: McGraw-Hill; 1999. pp. 407–22.
-
- Anderson MC. A text and atlas of integrated colposcopy. St. Louis: Mosby-Year Book; 1991.
-
- Critchlow CW, Wolner-Hanssen P, Eschenbach DA, et al. Determinants of cervical ectopia and of cervicitis: age, oral contraception, specific cervical infection, smoking, and douching. Am J Obstet Gynecol. 1995;173:534–43. - PubMed
-
- Harrison HR, Costin M, Meder JB, et al. Cervical Chlamydia trachomatis infection in university women: relationship to history, contraception, ectopy, and cervicitis. Am J Obstet Gynecol. 1985;153:244–51. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
