

Early diagnosis of candidemia in intensive care unit patients with sepsis: a prospective comparison of (1→3)-β-D-glucan assay, Candida score, and colonization index
- PMID: 22018278
- PMCID: PMC3334800
- DOI: 10.1186/cc10507
Early diagnosis of candidemia in intensive care unit patients with sepsis: a prospective comparison of (1→3)-β-D-glucan assay, Candida score, and colonization index
Abstract
Introduction: The culture-independent serum (1→3)-β-D-glucan (BG) detection test may allow early diagnosis of invasive fungal disease, but its clinical usefulness needs to be firmly established. A prospective single-center observational study was conducted to compare the diagnostic value of BG assay, Candida score (CS), and colonization index in intensive care unit (ICU) patients at risk for Candida sepsis.
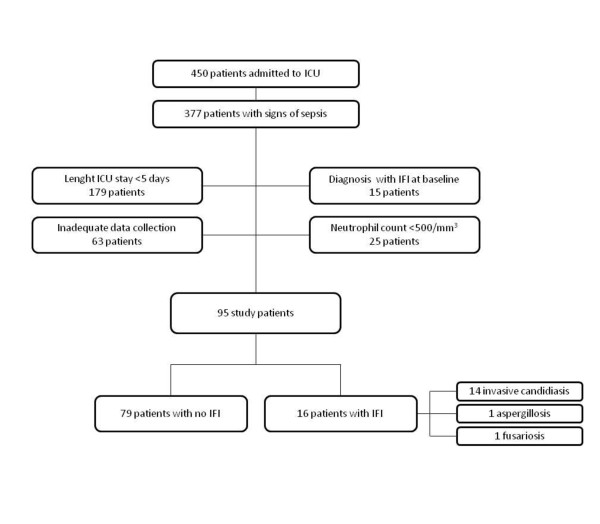
Methods: Of 377 patients, consecutively admitted to ICU for sepsis, 95 patients having an ICU stay of more than five days were studied. Blood specimens for fungal culture and BG measurement were obtained at the onset of clinical sepsis. For CS and colonization index calculations, surveillance cultures for Candida growth, and/or clinical data were recorded.
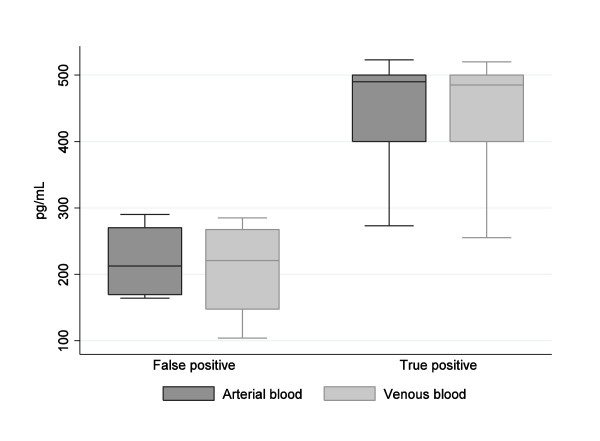
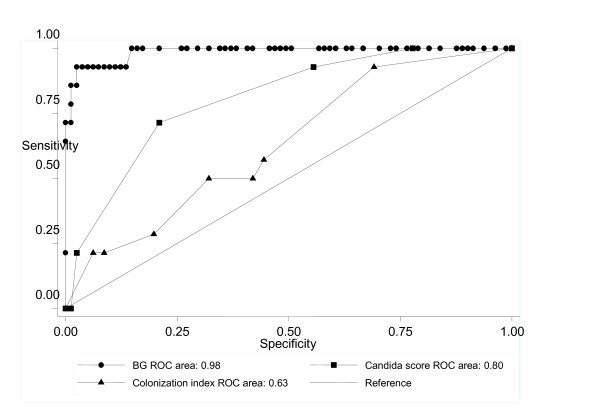
Results: Sixteen (16.8%) patients were diagnosed with proven invasive fungal infection, 14 with candidiasis (13 candidemia and 1 mediastinitis) and 2 with pulmonary aspergillosis or fusariosis. Of 14 invasive Candida-infection patients, 13 had a serum sample positive for BG, 10 had a CS value ≥ 3, and 7 a colonization index ≥ 0.5. In the 12 candidemic patients, a positive BG result was obtained 24 to 72 hrs before a culture-documented diagnosis of invasive candidiasis. The positive and negative predictive values for the BG assay were higher than those of CS and colonization index (72.2% versus 57.1% and 27.3%; and 98.7% versus 97.2% and 91.7%, respectively).
Conclusions: A single-point BG assay based on a blood sample drawn at the sepsis onset, alone or in combination with CS, may guide the decision to start antifungal therapy early in patients at risk for Candida infection.
Figures
Comment in
-
Is (1→3)-β-D-glucan the missing link from bedside assessment to pre-emptive therapy of invasive candidiasis?Crit Care. 2011;15(6):1017. doi: 10.1186/cc10544. Epub 2011 Dec 5. Crit Care. 2011. PMID: 22171793 Free PMC article.
References
-
- Marchetti O, Bille J, Fluckiger U, Eggimann P, Ruef C, Garbino J, Calandra T, Glauser MP, Täuber MG, Pittet D. Fungal Infection Network of Switzerland. Epidemiology of candidemia in Swiss tertiary care hospitals: secular trends, 1991-2000. Clin Infect Dis. 2004;38:311–320. doi: 10.1086/380637. - DOI - PubMed
-
- Leroy O, Gangneux JP, Montravers P, Mira JP, Gouin F, Sollet JP, Carlet J, Reynes J, Rosenheim M, Regnier B, Lortholary O. AmarCand Study Group. Epidemiology, management, and risk factors for death of invasive Candida infections in critical care: a multicenter, prospective, observational study in France (2005-2006) Crit Care Med. 2009;37:1612–1618. doi: 10.1097/CCM.0b013e31819efac0. - DOI - PubMed
-
- Kett DH, Azoulay E, Echeverria PM, Vincent JL. Extended Prevalence of Infection in ICU Study (EPIC II) Group of Investigators. Candida bloodstream infections in intensive care units: analysis of the extended prevalence of infection in a intensive care unit study. Crit Care Med. 2011;39:665–670. doi: 10.1097/CCM.0b013e318206c1ca. - DOI - PubMed
-
- Morrell M, Fraser VJ, Kollef MH. Delaying the empiric treatment of Candida bloodstream infection until positive blood culture results are obtained: a potential risk factor for hospital mortality. Antimicrob Agents Chemother. 2005;49:3640–3645. doi: 10.1128/AAC.49.9.3640-3645.2005. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
