

The electrophysiological cardiac ventricular substrate in patients after myocardial infarction: noninvasive characterization with electrocardiographic imaging
- PMID: 22018301
- PMCID: PMC3365586
- DOI: 10.1016/j.jacc.2011.07.029
The electrophysiological cardiac ventricular substrate in patients after myocardial infarction: noninvasive characterization with electrocardiographic imaging
Abstract
Objectives: The aim of this study was to noninvasively image the electrophysiological (EP) substrate of human ventricles after myocardial infarction and define its characteristics.
Background: Ventricular infarct border zone is characterized by abnormal cellular electrophysiology and altered structural architecture and is a key contributor to arrhythmogenesis. The ability to noninvasively image its electrical characteristics could contribute to understanding of mechanisms and to risk-stratification for ventricular arrhythmia.
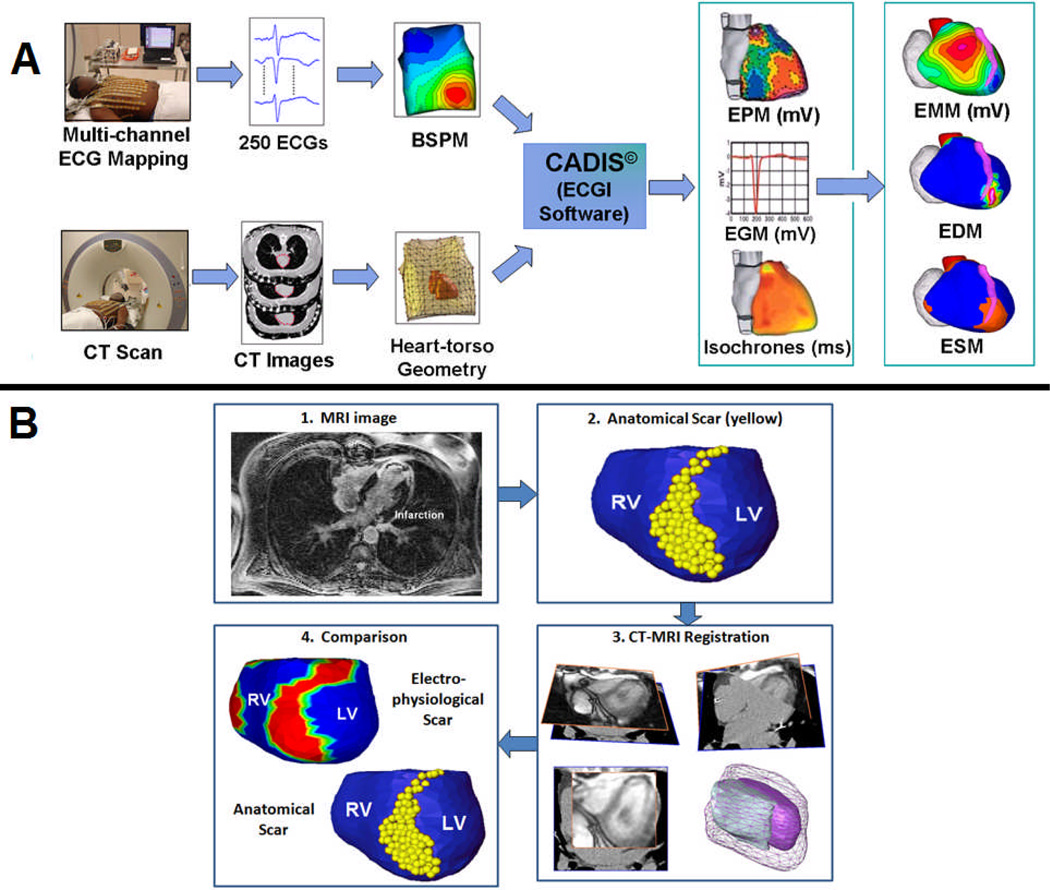
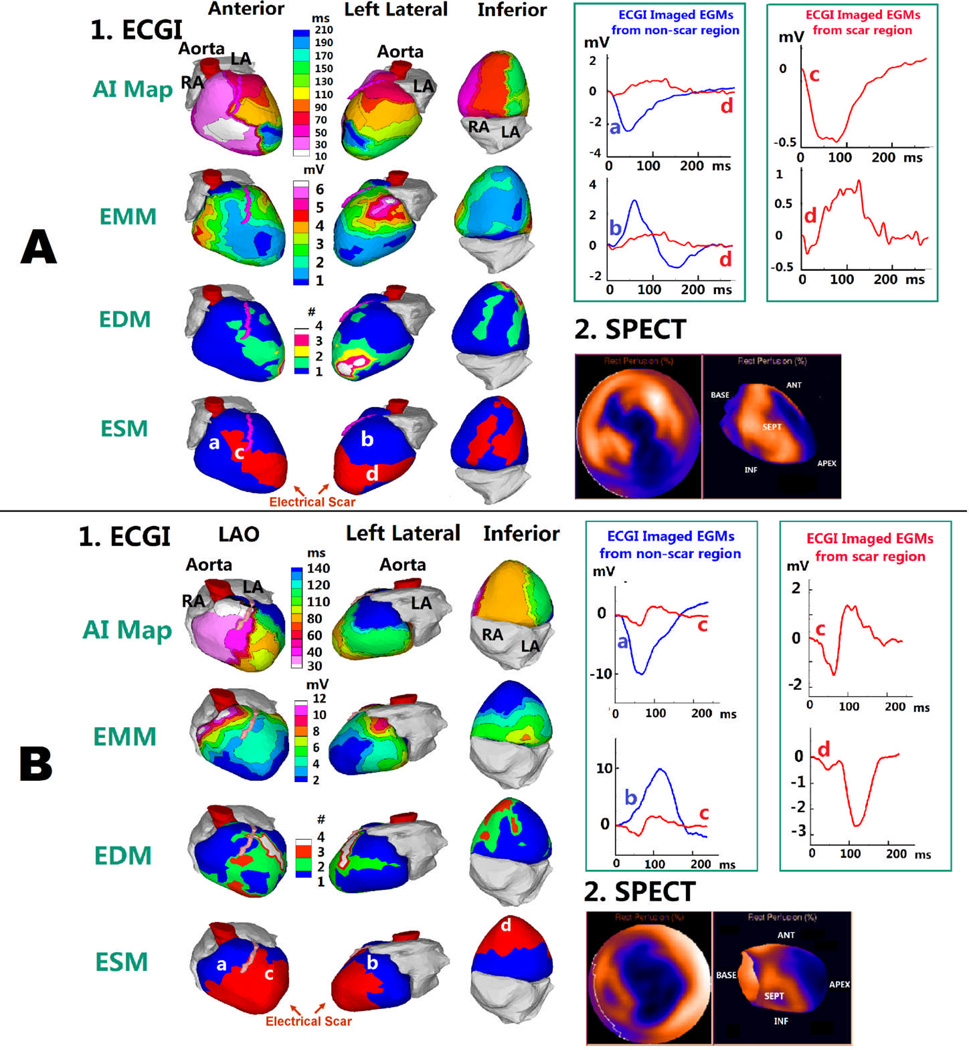
Methods: Electrocardiographic imaging, a noninvasive functional EP imaging modality, was performed during sinus rhythm (SR) in 24 subjects with infarct-related myocardial scar. The abnormal EP substrate on the epicardial aspect of the scar was identified, and its location, size, and morphology were compared with the anatomic scar imaged by other noninvasive modalities.
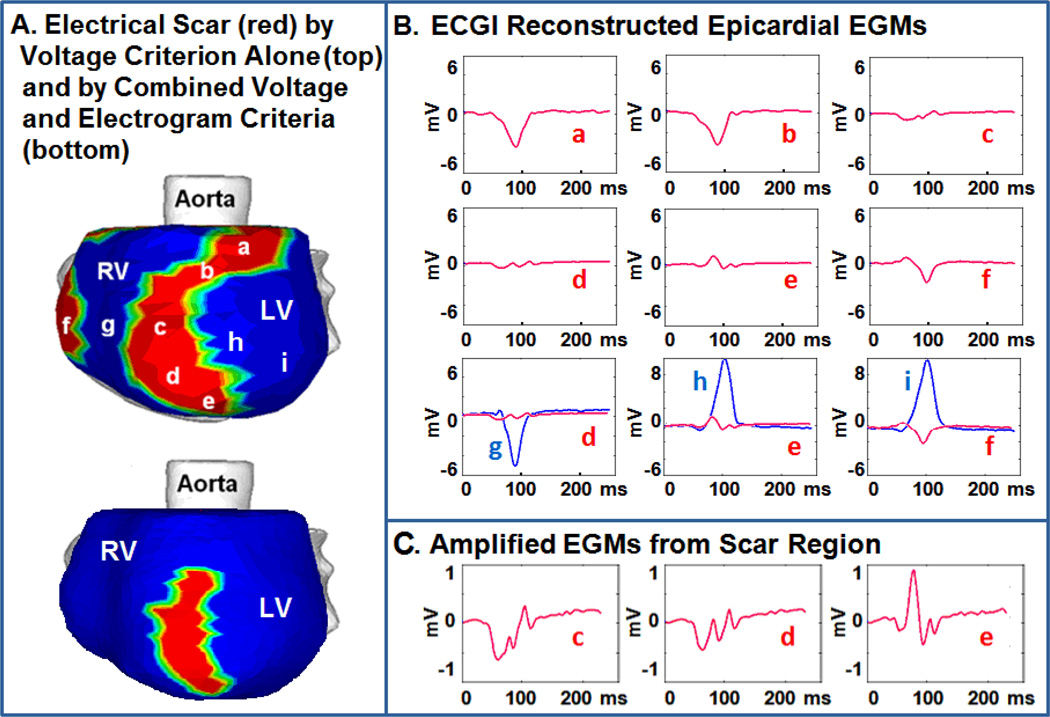
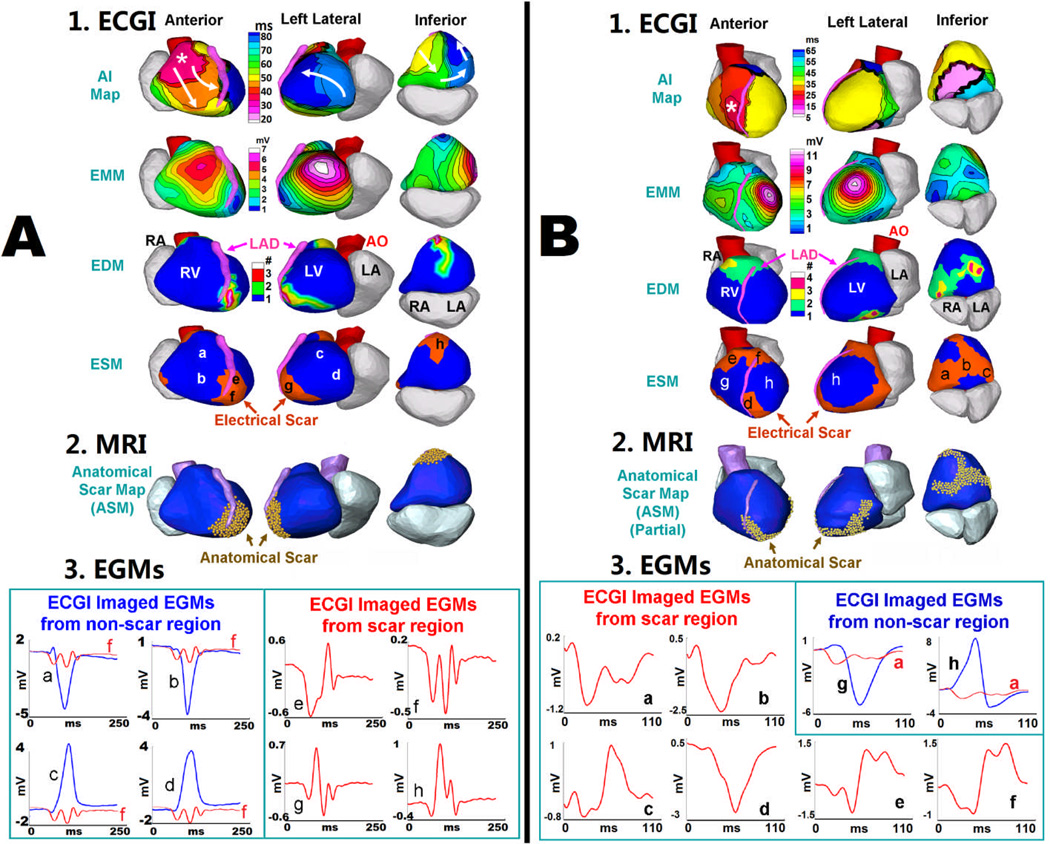
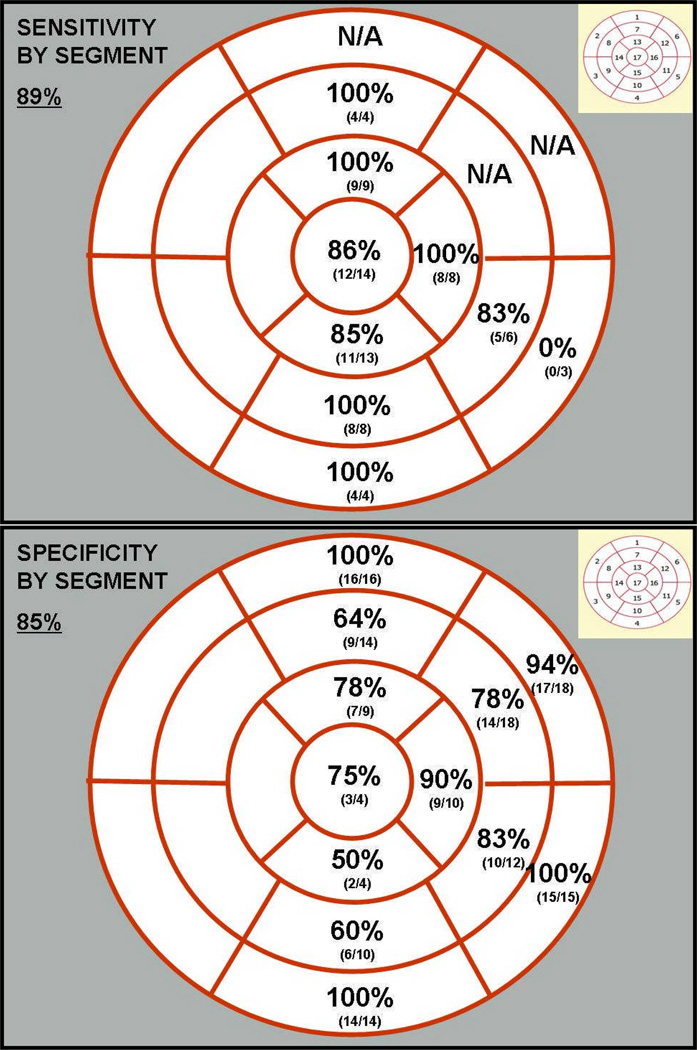
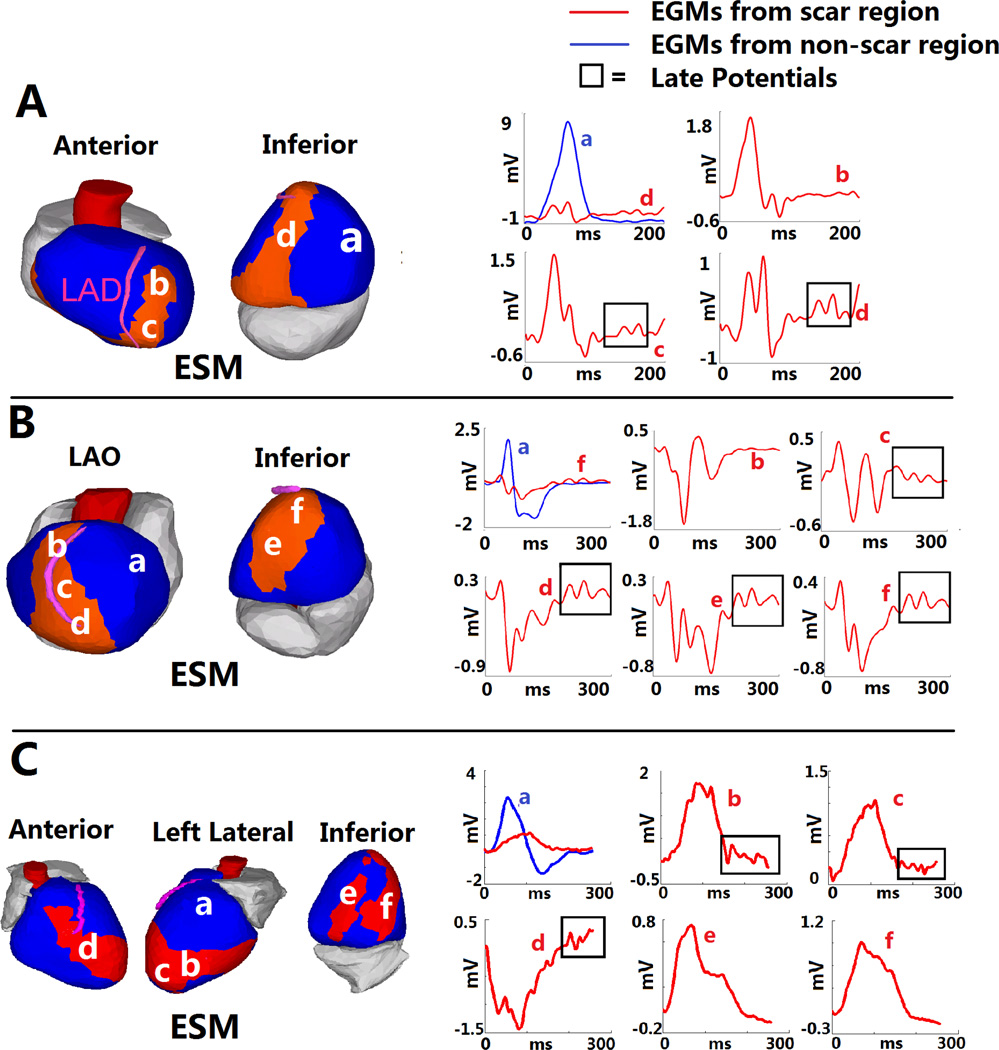
Results: Electrocardiographic imaging constructs epicardial electrograms that have characteristics of reduced amplitude (low voltage) and fractionation. Electrocardiographic imaging colocalizes the epicardial electrical scar to the anatomic scar with a high degree of accuracy (sensitivity 89%, specificity 85%). In nearly all subjects, SR activation patterns were affected by the presence of myocardial scar. Late potentials could be identified and were almost always within ventricular scar.
Conclusions: Electrocardiographic imaging accurately identifies areas of anatomic scar and complements standard anatomic imaging by providing scar-related EP characteristics of low voltages, altered SR activation, electrogram fragmentation, and presence of late potentials.
Copyright © 2011 American College of Cardiology Foundation. Published by Elsevier Inc. All rights reserved.
Figures
References
-
- Mahrholdt H, Wagner A, Holly TA, et al. Reproducibility of chronic infarct size measurement by contrast-enhanced magnetic resonance imaging. Circulation. 2002;106:2322–2327. - PubMed
-
- Bello D, Fieno DS, Kim RJ, et al. Infarct morphology identifies patients with substrate for sustained ventricular tachycardia. J Am Coll Cardiol. 2005;45:1104–1108. - PubMed
-
- Yan AT, Shayne AJ, Brown KA, et al. Characterization of peri-infarct zone by contrast-enhanced magnetic resonance imaging is a powerful predictor of post-myocardial infarction mortality. Circulation. 2006;114:32–39. - PubMed
-
- Peters NS, Wit AL. Myocardial architecture and ventricular arrhythmogenesis. Circulation. 1998;97:1746–1754. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
