

Immediate and delayed-onset systemic reactions after subcutaneous immunotherapy injections: ACAAI/AAAAI surveillance study of subcutaneous immunotherapy: year 2
- PMID: 22018614
- PMCID: PMC8207523
- DOI: 10.1016/j.anai.2011.05.020
Immediate and delayed-onset systemic reactions after subcutaneous immunotherapy injections: ACAAI/AAAAI surveillance study of subcutaneous immunotherapy: year 2
Abstract
Background: Incidences of subcutaneous immunotherapy (SCIT) related systemic reactions (SRs) and fatal reactions (FRs) are not well defined, nor are delayed-onset SRs and their treatment.
Objectives: To estimate SCIT-related SRs/FRs, and the incidence and treatment of delayed-onset SRs.
Methods: In 2008 and 2009, American Academy of Allergy, Asthma & Immunology (AAAAI) and American College of Allergy Asthma & Immunology (ACAAI) members completed a survey about SCIT-related SR severity (grade 1 = mild; grade 2 = moderate; grade 3 = severe anaphylaxis). In 2009, members reported the time of onset and use of epinephrine (EPI), with early onset defined as beginning ≤30 minutes, and delayed onset beginning more than 30 minutes after injections.
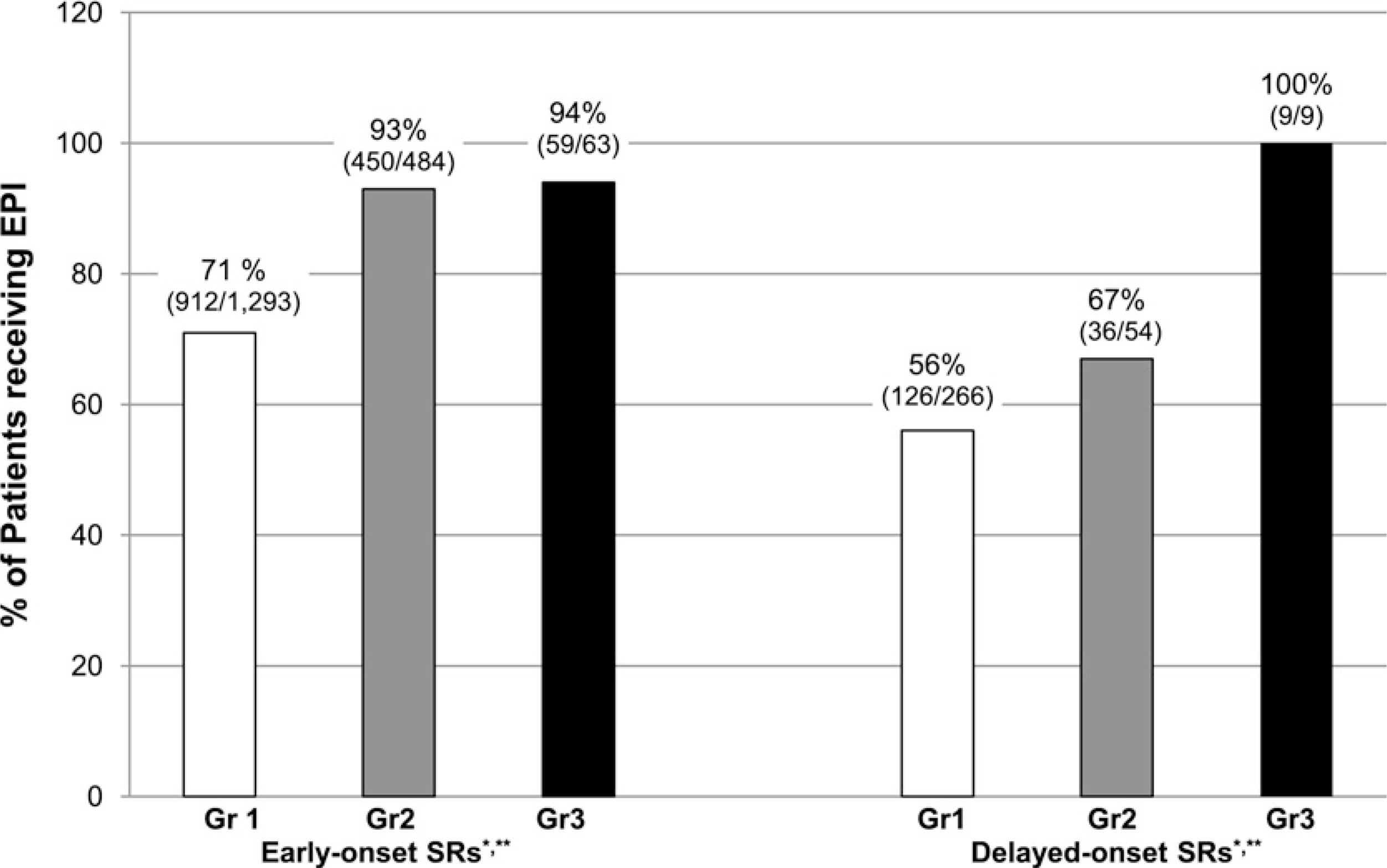
Results: As in year 1, no FRs were reported during year 2 (630 total practices responded). Among 267 practices providing data on the timing of SRs, 1,816 early-onset SRs (86%) and 289 (14%) delayed-onset SRs were reported. Fifteen percent (226/1,519) of grade 1, 10% (54/538) of grade 2, and 12.5% (9/72) of grade 3 SRs were delayed-onset. Among early-onset SRs, EPI was given for 71% of grade 1, 93% of grade 2, and 94% of grade 3s. Among delayed-onset SRs, EPI was given for 56% of grade 1, 67% of grade 2, and 100% of grade 3s (P = .0008 for difference in EPI administration based on severity; P = .07 based on time of onset).
Conclusions: Delayed-onset SRs are less frequent than previously reported. Epinephrine was given less frequently for grades 1 and 2 (but not grade 3) delayed-onset SRs compared with early-onset SRs. Further study of prescribing self-injectable EPI for SCIT patients in the event of delayed-onset SRs may be warranted.
Copyright © 2011 American College of Allergy. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Figures
References
-
- Lockey RF, Benedict LM, Turkeltaub PC, Bukantz SC. Fatalities from immunotherapy (IT) and skin testing (ST). J Allergy Clin Immunol. 1987;79:660–677. - PubMed
-
- Matloff SM, Bailit IW, Parks P, Madden N, Greineder DK. Systemic reactions to immunotherapy. Allergy Proc. 1993;14:347–350. - PubMed
-
- Moreno C, Cuesta-Herranz J, Fernandez-Tavora L, Alvarez-Cuesta E. Immunotherapy safety: a prospective multi-centric monitoring study of biologically standardized therapeutic vaccines for allergic diseases. Clin Exp Allergy. 2004;34:527–531. - PubMed
-
- Ragusa VF, Massolo A. Non-fatal systemic reactions to subcutaneous immunotherapy: a 20-year experience comparison of two 10-year periods. Eur Ann Allergy Clin Immunol 2004;36:52–55. - PubMed
-
- Reid MJ, Lockey RF, Turkeltaub PC, Platts-Mills TA. Survey of fatalities from skin testing and immunotherapy 1985–1989. J Allergy Clin Immunol. 1993;92:6–15. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
