

Major abdominal surgery in nursing home residents: a national study
- PMID: 22020197
- PMCID: PMC4477938
- DOI: 10.1097/SLA.0b013e3182383a78
Major abdominal surgery in nursing home residents: a national study
Abstract
Objective: To determine surgical risk in nursing home residents undergoing major abdominal surgery.
Background: Recent studies suggest that surgery can be performed safely in the very old. Surgical risk in nursing home residents is poorly understood.
Methods: We used national Medicare claims and the nursing home Minimum Data Set (1999-2006) to identify nursing home residents undergoing surgery (surgery for bleeding duodenal ulcer, cholecystectomy, appendectomy, and colectomy, n = 70,719). We compared operative mortality and use of invasive interventions (mechanical ventilation, intravascular hemodynamic monitoring, feeding tube placement, tracheostomy, and vena cava filters) among nursing home residents to rates among noninstitutionalized Medicare enrollees age 65 and older undergoing the same procedures. (n = 1,060,389). We adjusted for patient characteristics using logistic regression.
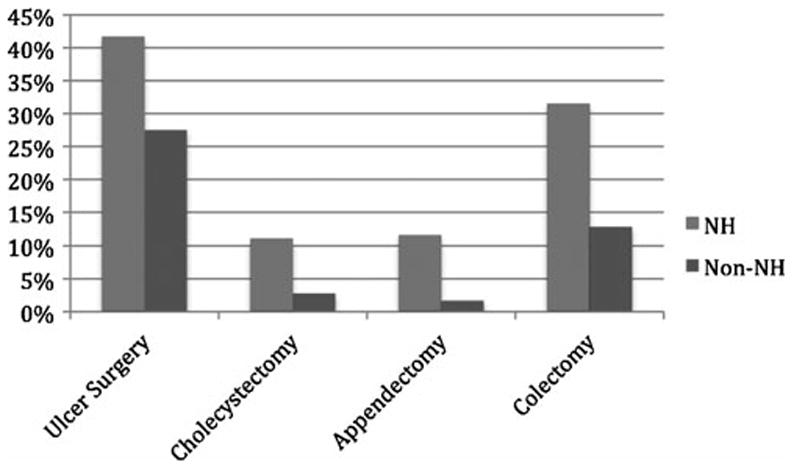
Results: Operative mortality among nursing home residents was substantially higher than among noninstitutionalized Medicare enrollees for all procedures (surgery for bleeding duodenal ulcer, 42% versus 26%, adjusted odds ratio (AOR) 1.79; colectomy, 32% versus 13%, AOR 2.06; appendectomy, 12% versus 2%, AOR 3.27; cholecystectomy, 11% versus 3%, AOR 2.65; P < 0.001 for all comparisons). Overall, invasive interventions were more common among nursing home residents than controls (ranging from 18% and 5%, respectively, for cholecystectomy to 55% and 43%, respectively, for surgery for bleeding duodenal ulcer, P < 0.0001 for all comparisons).
Conclusions: Nursing home residents experience substantially higher rates of mortality and invasive interventions after major surgery than other Medicare beneficiaries that are independent of age and measured comorbidities. Our data suggest that the risks of major surgery are substantially higher in nursing home residents and this information should inform decisions of physicians and patients and their families.
Figures
Comment in
-
Invited commentary on nursing home status is an independent risk factor for adverse 30-day postoperative outcomes after common, nonemergent inpatient procedures.Am J Surg. 2016 Aug;212(2):209-10. doi: 10.1016/j.amjsurg.2016.05.014. Epub 2016 Jul 1. Am J Surg. 2016. PMID: 27449210 No abstract available.
References
-
- Ibis C, Albayrak D, Hatipoglu AR, et al. The amount of comorbidities as a single parameter has no effect in predicting the outcome in appendicitis patients older than 60 years. South Med J. 2010;103(3):202–6. - PubMed
-
- Majeski J. Laparoscopic cholecystectomy in geriatric patients. Am J Surg. 2004;187:747–750. - PubMed
-
- Reissman p, Agachan F, Wexner Outcome of laparoscopic colorectal surgery in older patients. Am Surg. 1996;62(12):1060–3. - PubMed
-
- Gurevitch AJ, Davidovitch B, Kashtan H. Outcome of right colectomy for cancer in octogenarians. J Gastrointest Surg. 2009;13(1):100–4. - PubMed
-
- Massarweh NN, Legner VJ, Symons RG, et al. Impact of advancing age on abdominal surgical outcomes. Arch Surg. 2009;144(12):1108–1114. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
