

The changing pattern and implications of multiple organ failure after blunt injury with hemorrhagic shock
- PMID: 22020243
- PMCID: PMC3343366
- DOI: 10.1097/CCM.0b013e3182376e9f
The changing pattern and implications of multiple organ failure after blunt injury with hemorrhagic shock
Abstract
Objectives: To describe the incidence of postinjury multiple organ failure and its relationship to nosocomial infection and mortality in trauma centers using evidence-based standard operating procedures.
Design: Prospective cohort study wherein standard operating procedures were developed and implemented to optimize postinjury care.
Setting: Seven U.S. level I trauma centers.
Patients: Severely injured patients (older than age 16 yrs) with a blunt mechanism, systolic hypotension (<90 mm Hg), and/or base deficit (≥6 mEq/L), need for blood transfusion within the first 12 hrs, and an abbreviated injury score ≥2 excluding brain injury were eligible for inclusion.
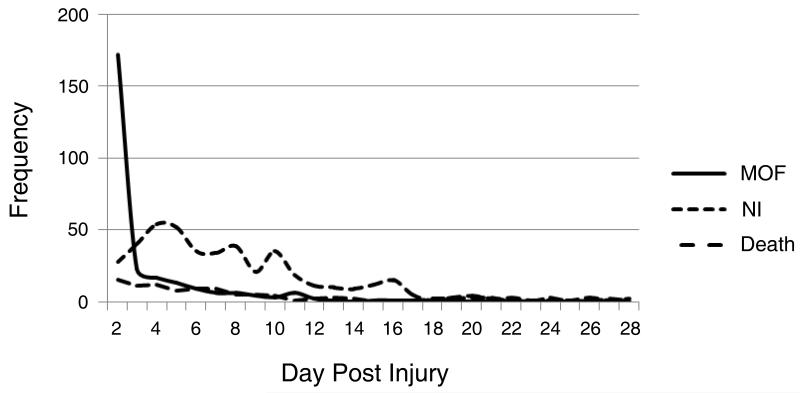
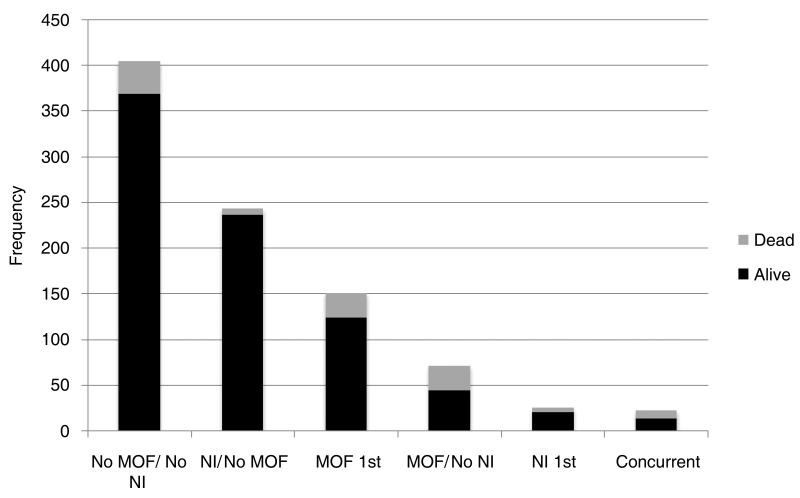
Measurements and main results: One thousand two patients were enrolled and 916 met inclusion criteria. Daily markers of organ dysfunction were prospectively recorded for all patients while receiving intensive care. Overall, 29% of patients had multiple organ failure develop. Development of multiple organ failure was early (median time, 2 days), short-lived, and predicted an increased incidence of nosocomial infection, whereas persistence of multiple organ failure predicted mortality. However, surprisingly, nosocomial infection did not increase subsequent multiple organ failure and there was no evidence of a "second-hit"-induced late-onset multiple organ failure.
Conclusions: Multiple organ failure remains common after severe injury. Contrary to current paradigms, the onset is only early, and not bimodal, nor is it associated with a "second-hit"-induced late onset. Multiple organ failure is associated with subsequent nosocomial infection and increased mortality. Standard operating procedure-driven interventions may be associated with a decrease in late multiple organ failure and morbidity.
Figures
Comment in
-
Hemorrhagic shock resuscitation: a critical issue on the development of posttraumatic multiple organ failure.Crit Care Med. 2012 Apr;40(4):1348-9. doi: 10.1097/CCM.0b013e31823e9501. Crit Care Med. 2012. PMID: 22425835 No abstract available.
References
-
- Baue AE. Multiple, progressive, or sequential systems failure. A syndrome of the 1970s. Arch Surg. 1975;110(7):779–781. - PubMed
-
- Eiseman B, Beart R, Norton L. Multiple organ failure. Surg Gynecol Obstet. 1977;144(3):323–326. - PubMed
-
- Acosta JA, Yang JC, Winchell RJ, et al. Lethal injuries and time to death in a level I trauma center. J Am Coll Surg. 1998;186(5):528–533. - PubMed
-
- Cuschieri J, Freeman B, O’Keefe G, et al. Inflammation and the host response to injury a large-scale collaborative project: patient-oriented research core standard operating procedure for clinical care X. Guidelines for venous thromboembolism prophylaxis in the trauma patient. J Trauma. 2008;65(4):944–950. - PMC - PubMed
-
- Evans HL, Cuschieri J, Moore EE, et al. Inflammation and the host response to injury, a Large-Scale Collaborative Project: patient-oriented research core standard operating procedures for clinical care IX. Definitions for complications of clinical care of critically injured patients. J Trauma. 2009;67(2):384–388. - PMC - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
