

Diagnostic and therapeutic approach of congenital solitary coronary artery fistulas in adults: Dutch case series and review of literature
- PMID: 22020997
- PMCID: PMC3077879
- DOI: 10.1007/s12471-011-0088-2
Diagnostic and therapeutic approach of congenital solitary coronary artery fistulas in adults: Dutch case series and review of literature
Abstract
Background: Coronary artery fistulas (CAFs) are infrequent anomalies, coincidentally detected during coronary angiography (CAG).
Aim: To elucidate the currently used diagnostic imaging modalities and applied therapeutic approaches.
Materials and methods: Five Dutch patients were found to have CAFs. A total of 170 reviewed subjects were subdivided into two comparable groups of 85 each, treated with either percutaneous 'therapeutic' embolisation (PTE group) or surgical ligation (SL group).
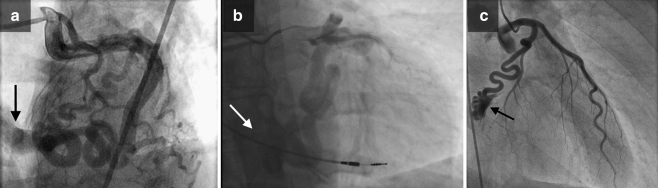
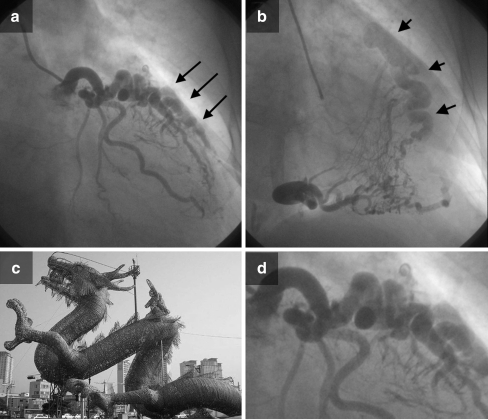
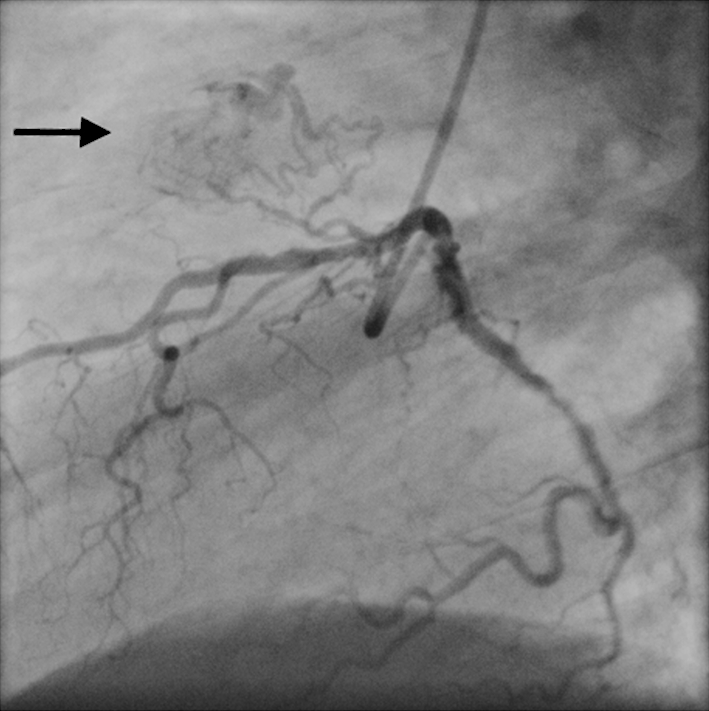
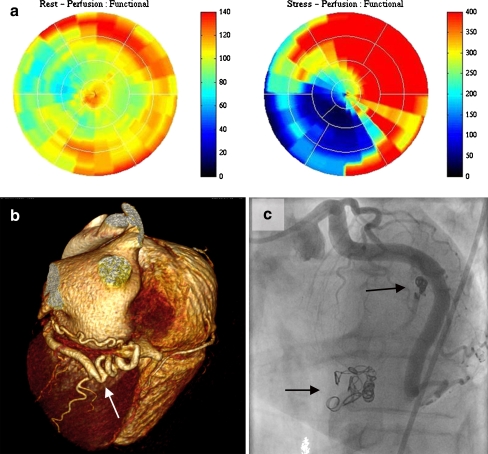
Results: In our series, the fistulas were visualised with several diagnostic imaging tests using echocardiography, multidetector computed tomography, and CAG. Four fistulas were unilateral and one was bilateral; five originated from the left and one originated from the right coronary artery. Among the reviewed subjects, high success rates were found in both treatment groups (SL: 97% and PTE: 93%). Associated congenital or acquired cardiovascular disorders were frequently present in the SL group (23%). Bilateral fistulas were present in 11% of the SL group versus 1% of the PTE group. The fistula was ligated surgically in one and abolished percutaneously in another. Medical treatment including metoprolol was conducted in two, and watchful waiting follow-up was performed in one.
Conclusions: Several diagnostic imaging techniques are available for assessment of the anatomical and functional characteristics of CAFs.
Figures
References
LinkOut - more resources
Full Text Sources
