

Review
doi: 10.2214/AJR.10.7260.
Cardiac masses, part 1: imaging strategies and technical considerations
Affiliations
- PMID: 22021530
- PMCID: PMC4382355
- DOI: 10.2214/AJR.10.7260
Item in Clipboard
Review
Cardiac masses, part 1: imaging strategies and technical considerations
AJR Am J Roentgenol.
2011 Nov.
Abstract
Objective: The objective of this article is to discuss optimal imaging strategies for the evaluation of cardiac masses. The advantages and disadvantages of echocardiography, cardiac MRI, gated cardiac CT, and nuclear imaging will be discussed and specific techniques presented.
Conclusion: Multimodality imaging plays a pivotal role in the diagnosis and surgical planning of cardiac masses. Clinical features, such as patient age, location, and imaging characteristics of the mass will determine the likely differential diagnosis.
Figures
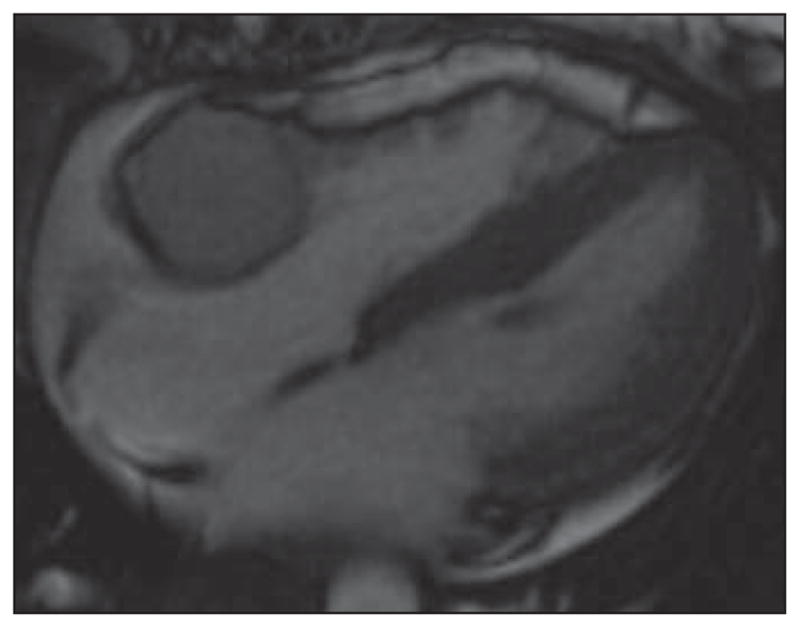
Steady-state free precession (SSFP) four-chamber image of heart in 37-year-old woman provides good anatomic information about cardiac morphology and can be used for functional assessment of cardiac motion and is typically acquired in multiple planes including two-, three-, and four-chamber cardiac planes. This is bright-blood imaging sequence with good endocardial-to-blood pool contrast ratio. In this patient, there is round mass in right atrioventricular groove that is isointense to myocardium of SSFP images, which have both T1 and T2 weighting that on subsequent imaging was confirmed to represent paraganglioma of atrioventricular groove. See also Figure S1, cine loop, in supplemental data online.
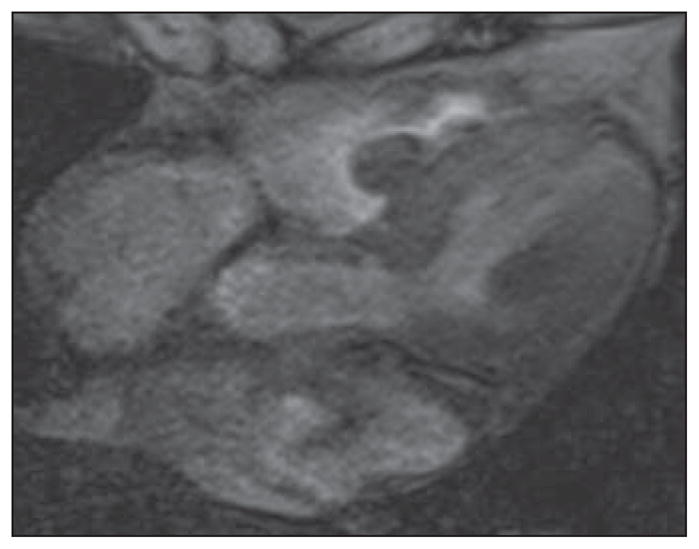
Gradient-echo MR images in four-chamber plane of heart in 82-year-old woman. These bright-blood images show lobulated mass in right ventricle subsequently resected and confirmed to represent myxoma. Contrast between endocardium and blood pool is less than on steady-state free precession (SSFP) cine sequences, and flow-related artifacts may be seen but this sequence is less susceptible to flow-related artifacts. See also Figure S2, cine loop, in supplemental data online.
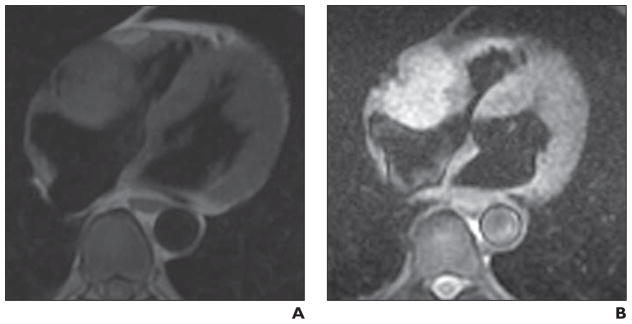
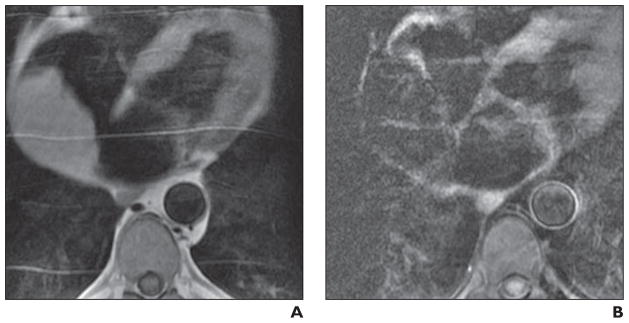
Imaging characteristics of phaeochromocytoma. A and B, Four-chamber black-blood T1-weighted (A) and T2-weighted (B) double inversion recovery images in 62-year-old man. These are high-resolution images that show mass relative to key adjacent structures. Mass is T1 isointense and T2 hyperintense to adjacent myocardium. Mass has imaging characteristics of phaeochromocytoma and was resected and confirmed to represent this diagnosis.
T1-weighted double inversion recovery four-chamber image of heart in 47-year-old man shows large epicardial mass adjacent to left ventricular lateral wall, which was metastasis from known germ cell tumor. Utility of high-resolution T1-weighted double inversion recovery imaging is high spatial resolution that allows determination that epicardial fat has not been invaded by tumor (arrow). When there is doubt, adding tagging sequences (Fig. S4, cine loop in supplemental data online) may better depict whether there is independent motion of a mass from myocardium.
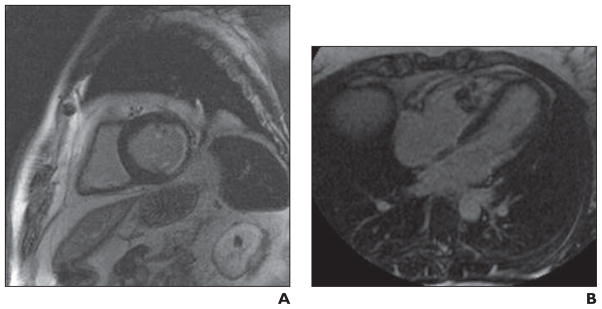
Large right atrial mass. A and B, Four-chamber T1-weighted double inversion recovery (A) and triple inversion recovery (B) cardiac MR images in 60-year-old man show mass is isointense on T1-weighted double inversion recovery images, and when fat saturation is applied to generate triple inversion recovery, mass loses signal homogeneously, consistent with lipoma.
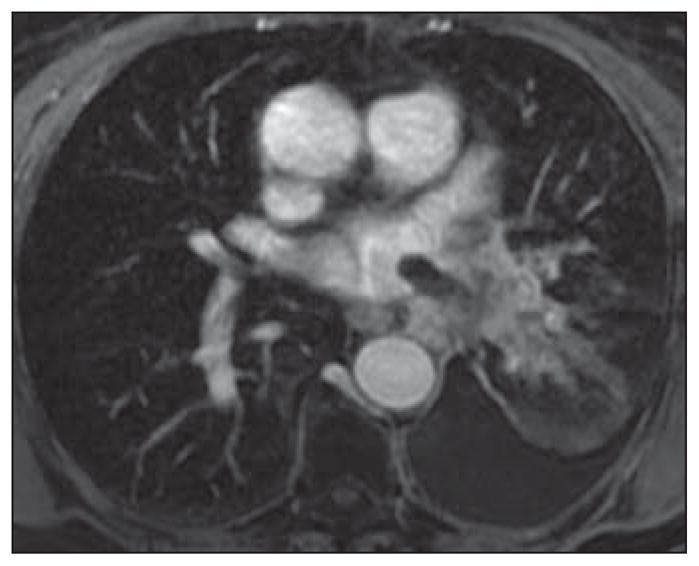
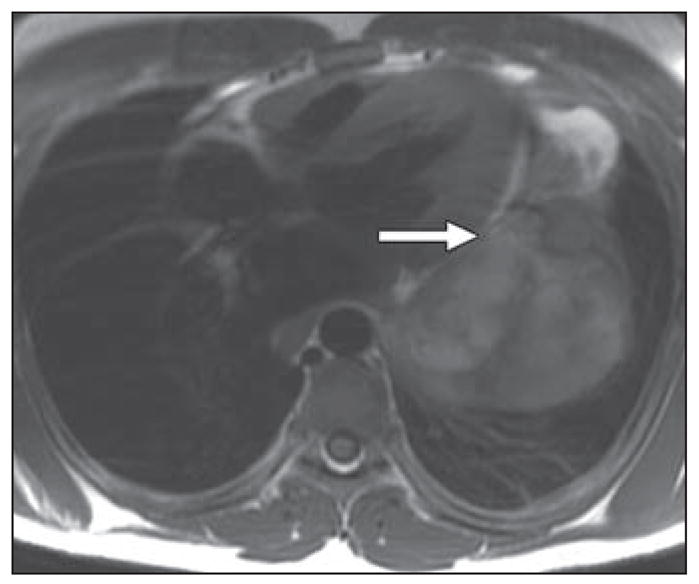
Contrast-enhanced volumetric interpolated breath-hold examination (VIBE) axial image of chest in 78-year-old woman with known primary adenocarcinoma of lung and worsening shortness of breath. There is extension of tumor along superior pulmonary vein with thumblike projection into vein and left atrium.
Myocardiac delayed enhancement imaging. Delayed enhancement cardiac MRI is typically acquired 10 minutes after weight-based dose of IV gadolinium with inversion time selected on turboFLASH (Siemens Healthcare) imaging to null signal from myocardium (typically in region of 300 milliseconds). Nulling myocardial signal is performed to better delineate areas of abnormal enhancement of myocardium. A, Myocardiac delayed enhancement imaging was initially described in imaging of myocardial scar after infarct. In this short-axis myocardiac delayed enhancement image there is subendocardial nontransmural delayed enhancement of myocardium in inferolateral basal myocardial segment, consistent with nontransmural infarct. In imaging of cardiac masses, myocardiac delayed enhancement imaging can be used to determine enhancement characteristics of mass and to differentiate mass from thrombus. B, Myocardiac delayed enhancement image shows heterogeneous enhancement of right ventricular mass in woman with history of sarcoma in calf. Right ventricular mass was resected and confirmed to represent metastasis.
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
