

Personalised medicine in Canada: a survey of adoption and practice in oncology, cardiology and family medicine
- PMID: 22021765
- PMCID: PMC3191410
- DOI: 10.1136/bmjopen-2011-000110
Personalised medicine in Canada: a survey of adoption and practice in oncology, cardiology and family medicine
Abstract
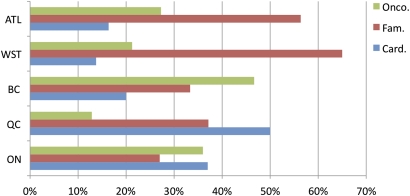
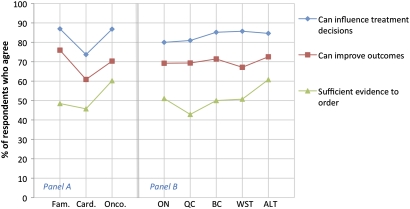
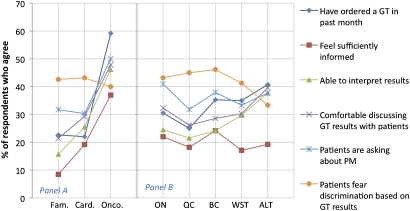
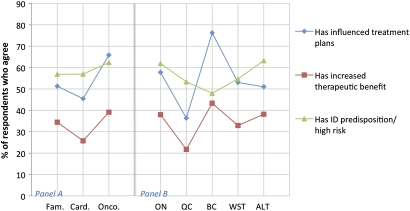
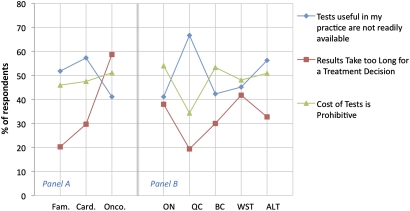
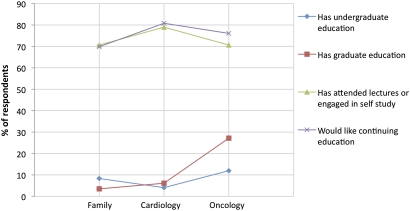
Introduction In order to provide baseline data on genetic testing as a key element of personalised medicine (PM), Canadian physicians were surveyed to determine roles, perceptions and experiences in this area. The survey measured attitudes, practice, observed benefits and impacts, and barriers to adoption. Methods A self-administered survey was provided to Canadian oncologists, cardiologists and family physicians and responses were obtained online, by mail or by fax. The survey was designed to be exploratory. Data were compared across specialties and geography. Results The overall response rate was 8.3%. Of the respondents, 43%, 30% and 27% were family physicians, cardiologists and oncologists, respectively. A strong majority of respondents agreed that genetic testing and PM can have a positive impact on their practice; however, only 51% agreed that there is sufficient evidence to order such tests. A low percentage of respondents felt that they were sufficiently informed and confident practicing in this area, although many reported that genetic tests they have ordered have benefited their patients. Half of the respondents agreed that genetic tests that would be useful in their practice are not readily available. A lack of practice guidelines, limited provider knowledge and lack of evidence-based clinical information were cited as the main barriers to practice. Differences across provinces were observed for measures relating to access to testing and the state of practice. Differences across specialties were observed for the state of practice, reported benefits and access to testing. Conclusions Canadian physicians recognise the benefits of genetic testing and PM; however, they lack the education, information and support needed to practice effectively in this area. Variability in practice and access to testing across specialties and across Canada was observed. These results support a need for national strategies and resources to facilitate physician knowledge, training and practice in PM.
Conflict of interest statement
Figures
References
-
- President's Council of Advisors on Science and Technology (PCAST). “Priorities for Personalized Medicine”. http://www.whitehouse.gov/files/documents/ostp/PCAST/pcast_report_v2.pdf (accessed Sep 2008).
-
- Ku CS, Loy EY, Salim A, et al. The discovery of human genetic variations and their use as disease markers: past, present and future. J Hum Genet 2010;55:403–15. - PubMed
LinkOut - more resources
Full Text Sources